{kind=link}
Diagnostic Challenges of Intracardiac “Ghost” Images Following ICD Explantation
The field of cardiac electrophysiology relies heavily on imaging to guide the removal of implantable cardioverter-defibrillators (ICDs). However, clinicians occasionally encounter diagnostic dilemmas when imaging reveals persistent, abnormal structures—often termed “ghosts”—within the cardiac chambers after the hardware has been removed. Understanding the nature of these findings is critical to patient safety and the prevention of unnecessary interventions.
Understanding the “Ghost” Phenomenon
An ICD system consists of a pulse generator and leads—insulated wires that transmit electrical signals between the heart and the device. Over time, these leads can become encapsulated by fibrous tissue, adhering to the endocardium or vascular walls. When a lead is extracted, a remnant of this fibrous sheath or a localized thrombus may remain, creating an artifact on diagnostic imaging that resembles the original hardware. Clinicians refer to these persistent structures as “ghosts.”
The Role of Multimodality Imaging
Distinguishing between an infectious vegetation, a benign thrombus, and a harmless fibrous remnant is a complex task. Relying on a single imaging modality is often insufficient. Current clinical practice emphasizes a multimodality approach to gather a comprehensive view of the intracardiac space:
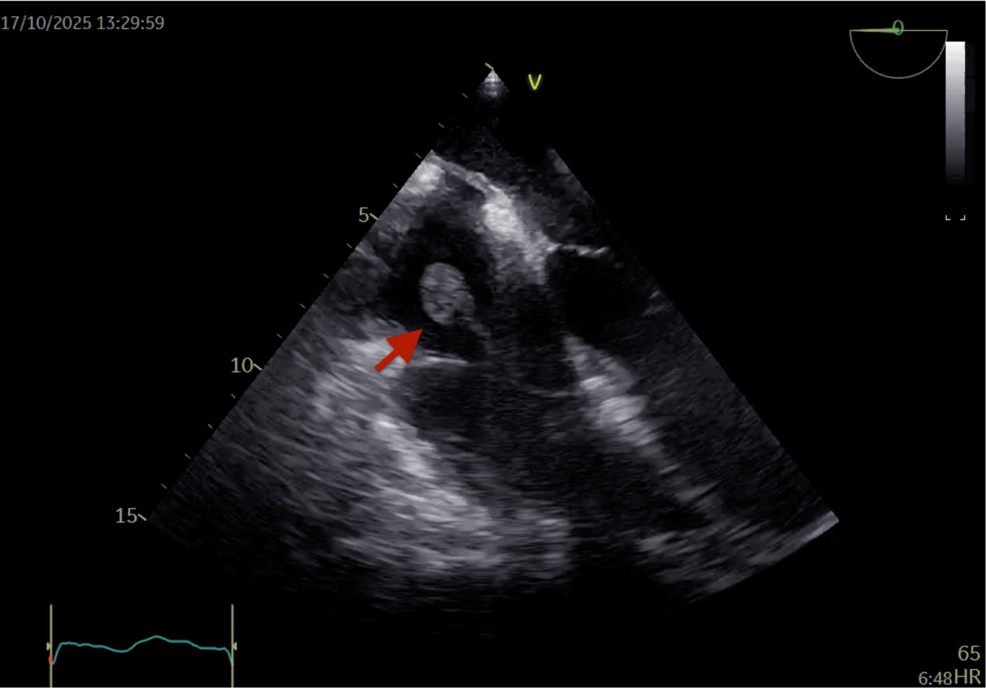
- Echocardiography (TTE/TEE): Transesophageal echocardiography (TEE) remains the gold standard for initial visualization of valvular and atrial structures due to its superior resolution compared to transthoracic imaging.
- Cardiac Computed Tomography (CT): Useful for assessing the anatomical relationship between the suspected mass and surrounding cardiac structures, particularly in identifying calcification or tethering.
- Cardiac Magnetic Resonance (CMR): Provides excellent tissue characterization, helping to differentiate between fibrous tissue and active inflammatory or infectious processes.
- Nuclear Imaging: Techniques such as PET/CT can be employed when there is a high clinical suspicion of device-related infection, as they highlight metabolic activity associated with inflammation.
Clinical Management and Decision Making
The discovery of an intracardiac mass post-explantation does not automatically necessitate surgical intervention. The management strategy is heavily dictated by the patient’s clinical presentation. If a patient remains asymptomatic and inflammatory markers—such as C-reactive protein (CRP) or white blood cell counts—are within normal limits, a conservative approach of surveillance imaging is often the preferred path.
Conversely, if the “ghost” is accompanied by systemic signs of infection, fever, or embolic events, aggressive diagnostic workup and potential surgical removal of the remnant may be required. The goal is to avoid the high morbidity associated with cardiac surgery whenever evidence suggests the mass is an inert, non-infectious fibrous remnant.
Key Takeaways for Practitioners
- Context is King: Always correlate imaging findings with the patient’s physical symptoms and laboratory results.
- Don’t Rush to Intervention: Many post-explantation masses are benign fibrous remnants that do not require surgical removal.
- Leverage Multimodality Imaging: Use a combination of TEE, CT, and advanced nuclear imaging to characterize the tissue before committing to a treatment plan.
Conclusion
As the number of ICD explantations increases, clinicians will continue to encounter these diagnostic challenges. The “ghost” image serves as a reminder that imaging is only one part of the clinical narrative. By utilizing a deliberate, multimodality diagnostic framework, physicians can provide more accurate assessments, sparing patients from the risks of invasive procedures when conservative management is safe and appropriate.
Frequently Asked Questions
What is an intracardiac “ghost”?
It is an imaging artifact, typically a fibrous tissue remnant or localized thrombus, that remains in the heart after an ICD lead has been extracted, appearing similar to the original lead on scans.
Is an intracardiac mass always dangerous?
No. While any mass in the heart requires investigation, many “ghosts” are simply harmless fibrous tissue left behind after lead removal and do not cause clinical symptoms.
How do doctors tell the difference between a thrombus and an infection?
Doctors use a combination of laboratory blood tests to check for systemic inflammation and advanced imaging like PET/CT scans to look for metabolic activity that typically signals an active infection.
Keep reading