{kind=link}
Understanding Cervico-Isthmic Pregnancy: Risks, Diagnosis, and Management
A cervico-isthmic pregnancy is a rare and potentially life-threatening form of ectopic implantation occurring in the lower uterine segment or the cervical canal. Unlike a typical intrauterine pregnancy, this condition carries a high risk of massive hemorrhage due to the vascular nature of the cervix and the lower uterine isthmus. According to the American College of Obstetricians and Gynecologists (ACOG), early ultrasound detection is critical for clinical management, as the condition frequently mimics other obstetric complications like placenta previa or threatened miscarriage.
What Defines a Cervico-Isthmic Pregnancy?
This condition occurs when a fertilized egg implants into the cervical canal or the isthmus—the narrow transition zone between the uterine body and the cervix. Because the cervical tissue lacks the contractile muscle fibers found in the uterine fundus, it cannot effectively constrict to stop bleeding after the placenta begins to detach. The National Institutes of Health (NIH) notes that this specific location is often associated with a high incidence of placenta accreta spectrum, where the placenta grows too deeply into the uterine wall, further increasing the risk of severe intraoperative blood loss during intervention.
How Is It Diagnosed?
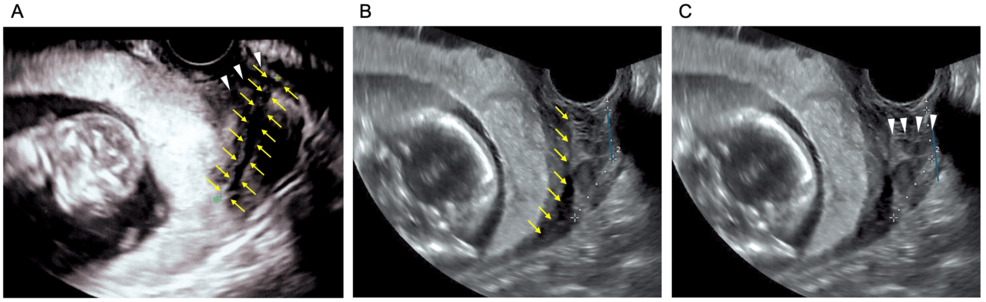
Diagnosis relies heavily on transvaginal ultrasound imaging. Clinicians look for specific markers, such as an empty uterine cavity, a gestational sac located below the level of the internal os, and a lack of a “sliding sign”—the ability to move the sac relative to the cervix during pressure from the ultrasound probe. According to research published in the Journal of Ultrasound in Medicine, clinicians must distinguish this from a low-lying intrauterine pregnancy that is simply aborting, as the management pathways for these conditions differ significantly.

Clinical Management and Treatment Options
Treatment strategies are tailored based on the patient’s hemodynamic stability, gestational age, and desire for future fertility. Standard approaches include:
- Medical Management: For stable patients, systemic or local injection of methotrexate may be used to terminate the pregnancy and induce resorption of the tissue.
- Surgical Intervention: Dilation and curettage is often avoided due to the extreme risk of hemorrhage. Instead, surgeons may use specialized techniques like cervical artery ligation or uterine artery embolization to reduce blood flow before removing the pregnancy.
- Hysterectomy: In cases of life-threatening hemorrhage or deeply invasive placenta accreta, an emergency hysterectomy remains the definitive, life-saving procedure.
Key Differences: Cervical vs. Isthmic Implantation
While often grouped together, these two sites present distinct clinical challenges. Cervical pregnancies are located entirely within the cervical canal, whereas isthmic pregnancies sit at the junction of the uterus and cervix. According to data from the American Journal of Obstetrics and Gynecology, isthmic pregnancies are more likely to involve the uterine vasculature, leading to higher rates of transfusion requirements compared to purely cervical implantations.
Frequently Asked Questions
- Is this the same as a tubal ectopic pregnancy?
- No. A tubal pregnancy occurs in the fallopian tubes, while a cervico-isthmic pregnancy is a form of cervical or low-uterine implantation. Both are considered ectopic as they occur outside the normal uterine cavity.
- What are the primary symptoms?
- The most common presentation is painless vaginal bleeding, often occurring in the first trimester. Some patients may remain asymptomatic until a routine ultrasound.
- Does this affect future fertility?
- The impact on fertility depends on the treatment used. Conservative management with methotrexate may preserve the uterus, but the risk of recurrence or future placental complications remains higher than in the general population.
The management of cervico-isthmic pregnancy requires a multidisciplinary team, including obstetricians, maternal-fetal medicine specialists, and interventional radiologists. Early identification through high-resolution imaging remains the best defense against the severe hemorrhage associated with this diagnosis. Patients concerned about symptoms should seek immediate evaluation at a facility equipped for high-risk obstetric emergencies.
Worth a look