{kind=link}
High-resolution impedance manometry (HRIM) is emerging as a critical diagnostic tool for identifying gastroesophageal reflux disease (GERD) in patients with obesity, particularly when traditional testing methods remain inconclusive. By simultaneously measuring esophageal pressure and bolus transit, HRIM provides a more precise assessment of esophageal function, helping clinicians differentiate between physiological symptoms and anatomical abnormalities often complicated by excess body mass.
Why Obesity Complicates GERD Diagnosis
Obesity is a well-established risk factor for GERD, largely due to increased intra-abdominal pressure that can compromise the lower esophageal sphincter (LES). According to the American College of Gastroenterology, patients with a high body mass index (BMI) frequently experience more severe reflux symptoms, including heartburn and regurgitation.
However, standard diagnostic tests like traditional manometry or basic pH monitoring can sometimes fail to capture the full picture. Excess adipose tissue around the abdomen can alter the mechanics of the diaphragm and esophageal hiatus, leading to "hidden" or atypical reflux patterns that standard equipment might miss.
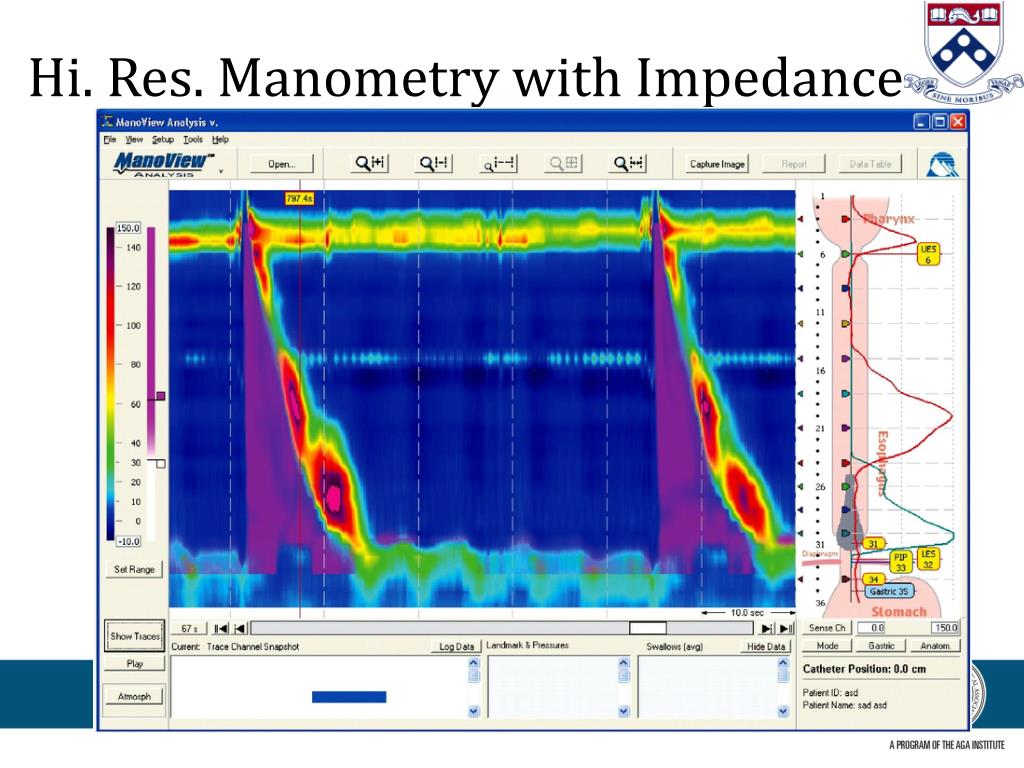
How HRIM Improves Diagnostic Accuracy
High-resolution impedance manometry improves upon older technology by using a higher density of sensors along the catheter. This allows gastroenterologists to create a "Clouse plot," a color-coded topographical map of esophageal pressure.
The addition of impedance monitoring—which detects the movement of liquid or gas within the esophagus—is the key to its effectiveness. As noted by the International Society for Diseases of the Esophagus, this dual-modality approach allows physicians to:
- Visualize Bolus Transit: See exactly how food and acid move through the esophagus in real-time.
- Identify Weakened Sphincters: Detect subtle failures in the LES that might be masked by the mechanical pressure of obesity.
- Assess Esophageal Motility: Evaluate whether the esophagus is clearing acid effectively, a function often impaired in patients with chronic reflux.
Clinical Implications for Treatment
For patients with obesity, the stakes for accurate diagnosis are high. Misdiagnosing or under-treating GERD can lead to complications such as Barrett’s esophagus or esophageal strictures.
By pinpointing the exact nature of the reflux, HRIM can help surgeons and gastroenterologists determine the most appropriate intervention. For example, if testing reveals that a patient’s reflux is driven by severe motility issues rather than just a weak sphincter, the surgical approach for weight loss or anti-reflux procedures may be modified to ensure long-term success.
Key Considerations for Patients
Patients experiencing persistent reflux symptoms—even after lifestyle modifications or standard medication—should consult with a gastroenterologist about advanced diagnostic options.
- Is HRIM invasive? The procedure involves passing a thin, flexible tube through the nose into the esophagus. While uncomfortable, it is generally well-tolerated and typically takes less than 30 minutes.
- Who is a candidate? Those with BMI-related reflux who have not responded to proton pump inhibitors (PPIs) or who are preparing for bariatric surgery are often the primary candidates for this testing.
As clinical practices shift toward more personalized medicine, the use of HRIM in the bariatric and gastroenterology populations represents a move toward objective, data-driven treatment plans that account for the unique anatomical challenges posed by obesity.
Related reading