{kind=link}
CRISPR-Edited Stem Cells Show Rapid Engraftment in High-Risk Leukemia Patients
A pioneering clinical trial using CRISPR/Cas9 gene-edited stem cells (trem-cel) has demonstrated rapid engraftment and promising early results in patients with high-risk acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS). The Phase 1/2 study, published in Nature, marks a significant advancement in precision oncology by combining CRISPR gene editing with allogeneic hematopoietic cell transplantation (alloHCT).
How the Therapy Works: Targeting CD33 to Protect Healthy Cells
The treatment, developed by Vor Biopharma, uses CRISPR/Cas9 to edit the CD33 gene in donor stem cells. CD33 is a protein expressed on AML and MDS cells but not on healthy hematopoietic stem cells (HSCs). By removing CD33 from the donor graft, trem-cel allows for:
- Selective targeting of leukemia cells with CD33-directed therapies (like gemtuzumab ozogamicin, or GO) without harming healthy blood cells.
- Reduced risk of graft-versus-host disease (GvHD) due to the minimal T-cell content in the graft.
- Potential for long-term remission by eliminating residual leukemia cells post-transplant.
The trial enrolled patients aged 18–70 with CD33-positive AML or MDS at high risk of relapse after alloHCT. Key eligibility criteria included:
- Adverse-risk genetics or minimal residual disease (MRD) positivity.
- An 8/8 HLA-matched donor.
- No prior autologous or allogeneic stem cell transplantation.
Rapid Engraftment and Safety Profile
The study reported 100% neutrophil engraftment by day 28 in evaluable patients, a critical milestone for alloHCT. Additional safety findings include:
Key Safety and Efficacy Metrics
- Neutrophil engraftment: Achieved in all evaluable patients by day 28.
- Platelet recovery: Median time to ≥20,000/µL platelets was 21 days.
- GvHD incidence: Low rates of grade 3–4 acute GvHD observed.
- CD33 editing: Persistent absence of CD33 on myeloid cells in peripheral blood and bone marrow.
- Relapse-free survival (RFS): Early data suggest potential for durable responses in high-risk patients.
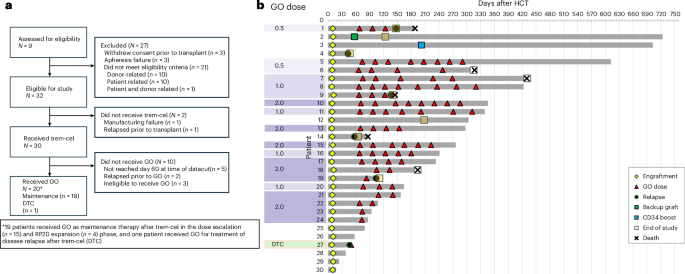
Study Design: A Two-Part Approach
The trial was structured in two phases:
Phase 1: Dose Escalation of GO Maintenance Therapy
Using a 3+3 design, researchers tested three dose levels of GO (0.5, 1.0 and 2.0 mg/m²) to determine the recommended phase 2 dose (RP2D). The maximum tolerated dose (MTD) was not reached, and the RP2D was established at 2.0 mg/m².
Phase 2: Dose Expansion
This phase assessed the safety and preliminary efficacy of the RP2D in a larger cohort. Patients received GO maintenance therapy for up to eight 28-day cycles. Those who relapsed or remained MRD-positive could enter a disease-targeted consolidation (DTC) protocol with intensified GO dosing.
“This approach represents a paradigm shift in how we treat high-risk leukemia. By editing the donor graft to remove CD33, we can use potent CD33-directed therapies without the risk of myelosuppression or GvHD.”
— Lead investigator (study protocol, Nature, 2026)
Why This Matters: Addressing Unmet Needs in AML
AML remains one of the most challenging cancers to treat, with relapse rates exceeding 50% in high-risk patients despite intensive chemotherapy and alloHCT. Current CD33-directed therapies, like GO, are limited by their toxicity to healthy blood cells. The trem-cel approach offers:
- Selective leukemia targeting: GO can now be used post-transplant without damaging the edited graft.
- Reduced GvHD risk: The graft contains fewer than 1×10⁶ CD3⁺ T cells/kg, lowering immune-mediated complications.
- Potential for MRD eradication: Early data suggest durable responses in patients with minimal residual disease.
Future Directions and Challenges
While the early results are encouraging, several questions remain:
- Long-term durability: Will CD33 editing persist in hematopoietic stem cells over years?
- Broader applicability: Can this approach be extended to other blood cancers or genetic diseases?
- Manufacturing scalability: How will CRISPR-edited grafts be produced at scale for widespread use?
The study authors emphasize the need for larger, randomized trials to confirm these findings. Vor Biopharma is also exploring combinations with other immunotherapies, such as CAR-T cells, to further enhance anti-leukemia activity.
Key Takeaways for Patients and Providers
- CRISPR-edited stem cells (trem-cel) show rapid and safe engraftment in high-risk AML/MDS patients.
- The therapy enables selective use of CD33-directed therapies post-transplant without myelosuppression.
- Early data suggest potential for durable remissions, but long-term follow-up is needed.
- This approach could reduce GvHD risk due to the minimal T-cell content in the graft.
- Further research is required to optimize dosing and combination strategies.
What’s Next?
Clinical trials for trem-cel are ongoing, with investigators recruiting patients for expanded cohorts. If you or a loved one has high-risk AML or MDS, consult your oncologist or hematologist about eligibility for these groundbreaking studies. For more information, visit:
FAQ: CRISPR-Edited Stem Cells for AML
1. How does CRISPR editing work in this therapy?
The CRISPR/Cas9 system precisely cuts the CD33 gene in donor stem cells, disabling its expression. This allows the edited cells to survive CD33-directed therapies while sparing healthy blood cells.
2. Who is eligible for this treatment?
Current eligibility includes adults (18–70) with CD33-positive AML or MDS at high risk of relapse, an HLA-matched donor, and no prior stem cell transplant. Specific genetic or disease criteria apply (e.g., adverse-risk genetics or MRD positivity).
3. What are the risks?
Risks include graft failure, infections, and GvHD, though early data suggest lower GvHD rates due to the T-cell-depleted graft. Long-term safety data are still being collected.
4. Is this therapy approved?
As of May 2026, trem-cel is not FDA-approved but is being evaluated in clinical trials. Approval would depend on further Phase 2/3 data.
5. How does this compare to standard alloHCT?
Standard alloHCT carries risks of GvHD and myelosuppression from CD33-directed therapies. Trem-cel avoids these issues by editing the graft to remove CD33, enabling safer post-transplant maintenance.
Related reading