{kind=link}
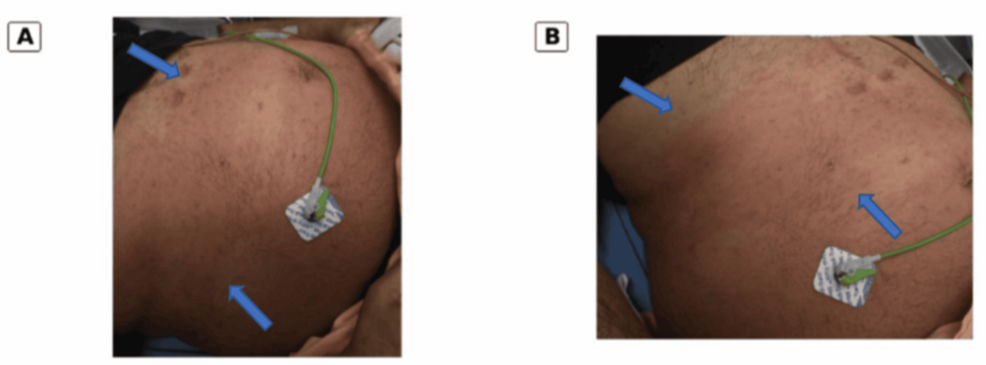
Cardiac allograft rejection typically presents with systemic symptoms like fatigue, dyspnea, or arrhythmias, but clinicians occasionally observe rare, cutaneous manifestations. Recent medical literature, including reports published in the journal Cureus, highlights that abdominal wall erythema—redness of the skin on the abdomen—can serve as an atypical, extracardiac indicator of rejection in heart transplant recipients. Recognizing these non-specific skin changes is essential for early diagnosis and timely intervention to prevent graft failure.
How Heart Transplant Rejection Manifests Cutaneously
While the gold standard for diagnosing cardiac allograft rejection remains endomyocardial biopsy, the immune system’s response to a donor heart can sometimes trigger secondary inflammatory processes elsewhere in the body. When a patient’s body begins to reject a donor organ, the resulting systemic inflammation can cause vascular changes.

According to research published in Cureus, localized inflammatory markers or immune complexes may settle in the skin, manifesting as erythematous patches. In the context of a heart transplant, any new, unexplained skin rash or persistent redness—particularly on the torso—should prompt immediate communication with a transplant team. These symptoms are often overlooked, yet they may signal that the patient’s immunosuppressive regimen requires adjustment.
Why Extracardiac Symptoms Are Often Misdiagnosed
Extracardiac manifestations of rejection are notoriously difficult to identify because they mimic common dermatological conditions like cellulitis or drug-induced rashes. Patients frequently present to primary care or emergency departments rather than their transplant center, which can lead to delays in specialized care.
- Diagnostic Difficulty: Skin redness is non-specific and can be caused by infections, allergic reactions, or medication side effects.
- The Transplant Context: Because transplant patients are on complex immunosuppression, they are at higher risk for opportunistic infections, which clinicians must rule out before attributing skin changes to graft rejection.
- Clinical Vigilance: Transplant centers emphasize that any change in physical appearance, even outside the chest or heart area, warrants a review of the patient’s current immunosuppressive therapeutic drug monitoring (TDM) levels.
Managing Potential Rejection Symptoms
When a patient presents with abdominal wall erythema after a heart transplant, the diagnostic process typically involves a multi-disciplinary approach. Cardiologists and dermatologists often collaborate to distinguish between an infectious process and an immune-mediated rejection event.

Medical teams usually prioritize the following steps:
- Biopsy of the skin lesion: This helps rule out common infectious or malignant causes.
- Echocardiography: Doctors use this to assess the structural function of the heart and check for fluid buildup or reduced contractility.
- Endomyocardial Biopsy: This remains the definitive test if clinical suspicion of rejection is high, as reported by the International Society for Heart and Lung Transplantation (ISHLT) guidelines.
Key Considerations for Transplant Recipients
Patients should not ignore skin changes, as they can be part of a broader systemic response. Early identification of rejection symptoms significantly improves the prognosis of the graft. If you are a transplant recipient, maintain a low threshold for reporting new skin lesions to your transplant coordinator.
Tracking the timing of these symptoms in relation to your medication schedule can provide your medical team with valuable data. While abdominal wall erythema is a rare finding, it serves as a reminder that the post-transplant patient requires vigilant, holistic monitoring to ensure the long-term viability of the donor heart.
Worth a look