{kind=link}
Acute Fatty Liver of Pregnancy: Recognizing a Rare Obstetric Emergency
Acute Fatty Liver of Pregnancy (AFLP) is a rare, life-threatening obstetric complication characterized by microvesicular fatty infiltration of hepatocytes. According to the American College of Obstetricians and Gynecologists (ACOG), the condition typically presents in the third trimester or early postpartum period. Because symptoms often mimic other conditions like preeclampsia or viral hepatitis, prompt diagnosis through clinical assessment and laboratory testing is essential to prevent maternal and fetal mortality.
What Causes Acute Fatty Liver of Pregnancy?
AFLP stems from a defect in mitochondrial fatty acid beta-oxidation in the fetus. The most common underlying mechanism is a deficiency in the enzyme long-chain 3-hydroxyacyl-CoA dehydrogenase (LCHAD), often linked to a mutation in the HADHA gene. When the fetus lacks this enzyme, toxic long-chain fatty acid intermediates accumulate and cross the placenta into the maternal circulation. According to the National Center for Biotechnology Information (NCBI), these fatty acids cause maternal liver dysfunction, which can rapidly progress to liver failure, coagulopathy, and multi-organ system involvement if not managed immediately.
Recognizing the Symptoms
Early symptoms of AFLP are often nonspecific, which can delay diagnosis. Patients frequently report:
- Persistent nausea and vomiting
- Abdominal pain, particularly in the right upper quadrant
- Jaundice (yellowing of the skin or eyes)
- Malaise and fatigue
- Polydipsia (excessive thirst) and polyuria
As the condition progresses, patients may develop severe complications, including hypoglycemia, elevated liver enzymes, and disseminated intravascular coagulation (DIC). Clinical guidelines from the Royal College of Obstetricians and Gynaecologists (RCOG) emphasize that any pregnant patient presenting with jaundice or persistent vomiting in the late third trimester should be evaluated for AFLP.
How is AFLP Diagnosed and Treated?
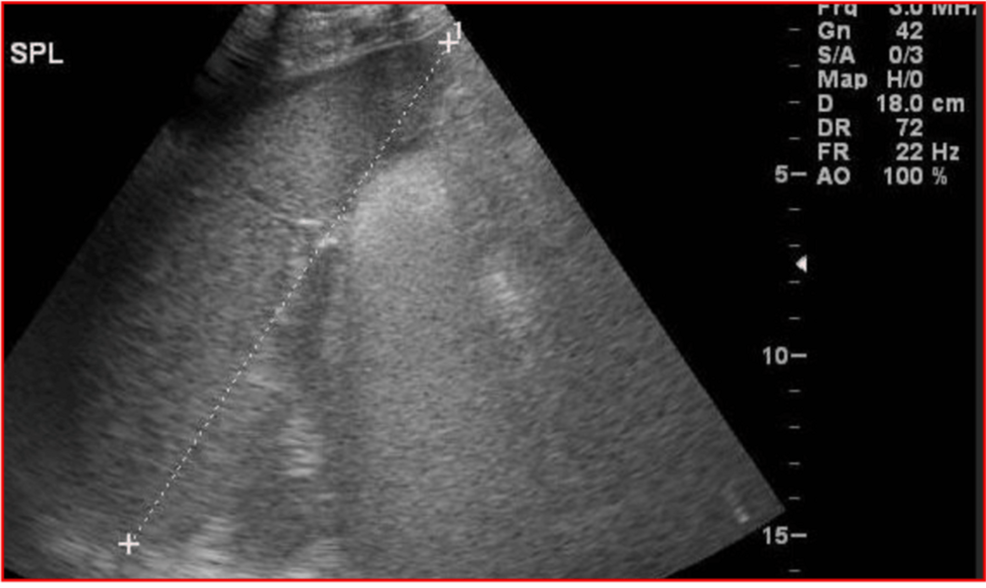
Diagnosis relies on a combination of clinical suspicion and laboratory findings. Physicians typically use the Swansea Criteria to confirm the diagnosis, which evaluates factors such as elevated uric acid, low fibrinogen, elevated bilirubin, and leukocytosis. Imaging, such as ultrasound or CT, is occasionally used, though it is not always sensitive enough to detect the microvesicular fat accumulation.
The definitive treatment for AFLP is immediate delivery of the fetus. According to the Mayo Clinic, delaying delivery to allow for fetal lung maturity can be dangerous for the mother. Post-delivery, the focus shifts to intensive supportive care, including:
- Correction of hypoglycemia with intravenous dextrose
- Management of coagulopathy through blood product replacement
- Monitoring for renal or hepatic failure
Comparison of Pregnancy-Related Liver Disorders
Differentiating AFLP from other pregnancy-specific liver conditions is critical for appropriate management. The following table highlights key differences based on clinical data from the American Association for the Study of Liver Diseases (AASLD):
| Condition | Typical Timing | Primary Clinical Feature |
|---|---|---|
| AFLP | Third Trimester | Liver failure, coagulopathy, hypoglycemia |
| HELLP Syndrome | Third Trimester | Hemolysis, elevated liver enzymes, low platelets |
| Intrahepatic Cholestasis | Second/Third Trimester | Severe pruritus (itching), elevated bile acids |
What is the Prognosis?
While AFLP was historically associated with high mortality rates, early recognition and advancements in critical care have significantly improved outcomes. According to data published in The Lancet, maternal mortality has dropped to less than 5% with prompt delivery and supportive management. However, the condition remains a medical emergency. Patients who recover from an initial episode of AFLP are encouraged to undergo genetic counseling, as the underlying LCHAD deficiency is an autosomal recessive disorder, meaning future pregnancies carry a risk of recurrence or fetal complications.
Worth a look