{kind=link}
Antibiotic-Associated Neuropsychiatric Symptoms: Understanding Drug-Induced Delirious Mania
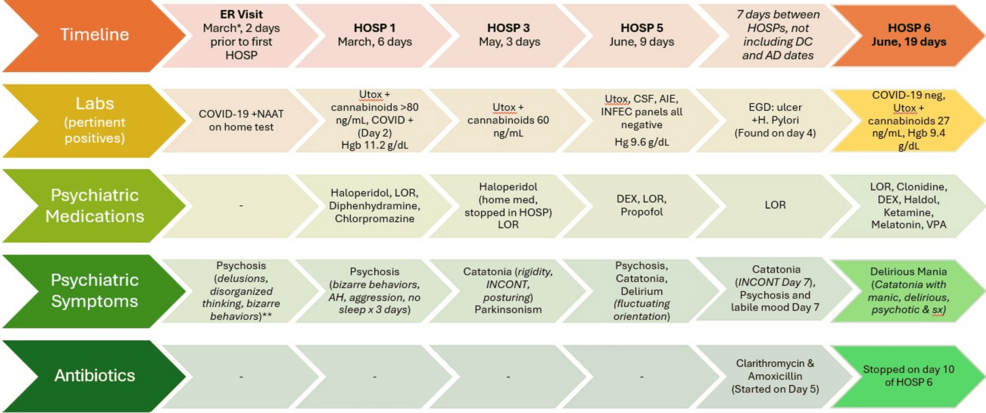
Research indicates that common antibiotics, including amoxicillin and clarithromycin, may rarely trigger neuropsychiatric adverse events, such as delirious mania, in vulnerable patients. While these medications are widely prescribed for bacterial infections, clinical reports highlight the importance of monitoring for sudden behavioral changes, particularly in adolescents with pre-existing psychiatric conditions. According to the National Library of Medicine, clinicians should maintain a high index of suspicion when psychiatric symptoms emerge shortly after initiating antibiotic therapy.
Pharmacological Mechanisms and Neuropsychiatric Risks
The link between antibiotic use and psychiatric symptoms—often termed “antibiotic-associated delirium”—remains a subject of ongoing clinical study. Clarithromycin, a macrolide antibiotic, is known to cross the blood-brain barrier and can interact with various neurotransmitter pathways, including GABAergic and glutamatergic systems.
According to data published in Cureus, the combination of amoxicillin and clarithromycin may alter the delicate chemical balance in the brain. In cases involving adolescents with a history of recurrent catatonia or psychosis, the introduction of these agents has been observed to coincide with the onset of acute delirious mania. Delirious mania is characterized by a rapid escalation of energy, disorganized thinking, and confusion, distinct from primary bipolar disorder or schizophrenia. Experts suggest that the inflammatory response to an underlying infection, coupled with the metabolic impact of the antibiotics, may lower the threshold for these neurotoxic reactions.
Clinical Monitoring for Vulnerable Populations
Adolescents with underlying neurodevelopmental or psychiatric diagnoses face a higher risk for adverse drug reactions. The U.S. Food and Drug Administration (FDA) emphasizes that healthcare providers should conduct a thorough medication reconciliation before prescribing antibiotics to patients with complex psychiatric histories.
When prescribing, clinicians are advised to:
- Review the patient’s full psychiatric and medical history for sensitivities.
- Educate caregivers to observe for sudden shifts in mood, sleep patterns, or cognitive clarity.
- Consider the potential for drug-drug interactions, particularly if the patient is already taking psychotropic medications like mood stabilizers or antipsychotics.
- Discontinue the offending agent promptly if symptoms of delirium emerge, as these reactions are often reversible upon the withdrawal of the drug.
Distinguishing Infection from Medication Side Effects
A primary challenge in clinical practice is distinguishing whether psychiatric symptoms are the result of the infection itself—such as systemic inflammation—or a direct side effect of the antibiotic treatment. Systemic infections can cause delirium, especially in younger populations. However, when symptoms escalate specifically following the administration of a new antibiotic regimen, drug-induced etiology becomes a priority consideration for medical teams.
According to reports in the American Psychiatric Association journals, clinicians often employ a “washout” period or switch to an alternative class of antibiotics to determine if the psychiatric symptoms resolve. This clinical strategy helps confirm the diagnosis and prevents unnecessary, long-term psychiatric interventions for a transient, medication-induced event.
Summary of Considerations
While antibiotics remain essential for treating bacterial infections, the potential for neuropsychiatric side effects should not be overlooked. For patients with a history of catatonia or psychosis, the risk-benefit ratio of specific antibiotics like clarithromycin warrants careful assessment. Future clinical research is needed to better identify biomarkers that predict which patients are most susceptible to these rare but significant neurotoxic reactions.
Key Takeaways for Patients and Families
- Monitor Closely: Watch for sudden changes in behavior, confusion, or agitation after starting any new medication.
- Communicate History: Always inform prescribing physicians about a patient’s full psychiatric history, including past episodes of catatonia or psychosis.
- Seek Prompt Care: If a patient exhibits signs of delirium, contact the prescribing physician immediately rather than waiting for the course of antibiotics to conclude.
- Review Medications: Consult with a pharmacist or physician regarding potential interactions between antibiotics and existing daily medications.