{kind=link}
Metabolic and Bariatric Surgery: Treating Obesity and MASLD
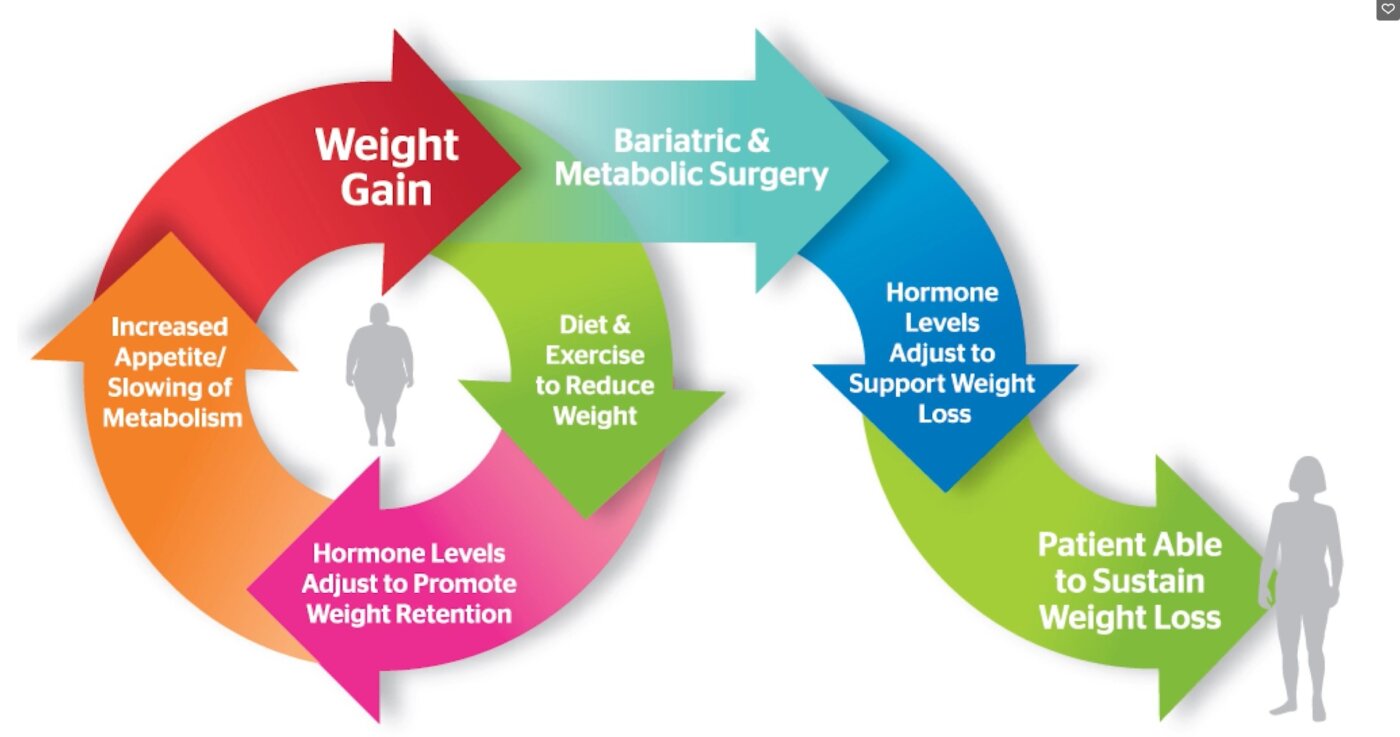
Metabolic and bariatric surgery (MBS) has evolved into a well-established intervention for individuals with class III obesity and class II obesity with comorbidities. Beyond significant and sustained weight loss, these procedures are increasingly recognized for their ability to treat associated disorders of metabolic function, specifically metabolic dysfunction-associated steatotic liver disease (MASLD).
- Laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass are the most common MBS procedures.
- MBS is suggested as the only definitive treatment for MASLD, a prevalent comorbidity of obesity.
- Research indicates that preoperative MASLD does not significantly hinder postoperative weight loss outcomes.
- Bariatric surgery can lead to the regression of hepatic steatosis and fibrosis.
Commonly Performed Bariatric Procedures
While various surgical options exist, laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass are the most frequently performed metabolic and bariatric surgical procedures worldwide. These interventions aim to provide a comprehensive treatment approach for both obesity and the metabolic dysfunctions that often accompany it.
Addressing Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD)
MASLD is a common condition in patients with severe obesity. Because of its prevalence and impact, metabolic bariatric surgery is suggested as the only definitive treatment for this condition. Recent clinical data highlights the significant impact of these surgeries on liver health:
Impact on Liver Stiffness and Steatosis
Using non-invasive monitoring tools like Fibroscan, researchers have observed profound improvements in liver health following surgery. In one prospective study of 111 patients, the following results were observed by seven months postoperatively:

- Reduction in MASLD: The prevalence of MASLD decreased from 100% preoperatively to 61% postoperatively.
- Fibrosis Improvement: Hepatic fibrosis decreased from 41% to 8%.
- Severe Fibrosis Resolution: Among patients with severe fibrosis (LSM > 12 kPa), 72% demonstrated resolution.
- Quantitative Metrics: There was a imply reduction in the Controlled Attenuation Parameter (CAP) of 26% and a mean reduction in Liver Stiffness Measurement (LSM) of 33%.
Does Preoperative MASLD Affect Weight Loss?
There have been concerns that patients with MASLD might experience altered weight loss patterns compared to those without the condition. Still, research involving 347 patients who underwent MBS between 2020 and 2024 suggests that preoperative MASLD does not significantly influence weight loss outcomes after Roux-en-Y gastric bypass or sleeve gastrectomy. When adjusting for factors such as age, sex, diabetes history, and baseline BMI, the overall weight loss patterns remained statistically similar between the MASLD and no-MASLD groups.
Managing Post-Surgical Complications
Despite advancements in surgical techniques, complications associated with metabolic and bariatric surgery are common and can occur long after the initial procedure. Gastroenterologists play a critical role in the long-term management and understanding of these complications to ensure patient safety and sustained health improvements.
Frequently Asked Questions
What is the difference between bariatric and metabolic surgery?
While often used interchangeably, bariatric surgery focuses on weight loss, while metabolic surgery emphasizes the improvement of metabolic disorders, such as type 2 diabetes and MASLD.
Can bariatric surgery actually cure liver fibrosis?
Studies show that bariatric surgery is associated with an improvement and, in many cases, total regression of MASLD and hepatic fibrosis. However, “resolution” in these contexts often refers to the normalization of CAP and LSM scores rather than histological resolution.
Which surgery is better for MASLD?
Both Roux-en-Y gastric bypass (RYGB) and sleeve gastrectomy (SG) have shown effectiveness. Current evidence suggests that preoperative MASLD does not significantly change the weight loss outcomes for either of these two common procedures.
Conclusion
Metabolic and bariatric surgery offers a powerful tool for treating severe obesity and its associated comorbidities. The evidence underscores its effectiveness not only in inducing profound weight loss but similarly in reversing the progression of metabolic dysfunction-associated steatotic liver disease. As surgical techniques continue to advance, the focus remains on long-term monitoring to manage complications and maintain the metabolic benefits achieved post-surgery.
Related reading