{kind=link}
The Balance of Care: Reducing Glucocorticoid Exposure in Pediatric Classic CAH
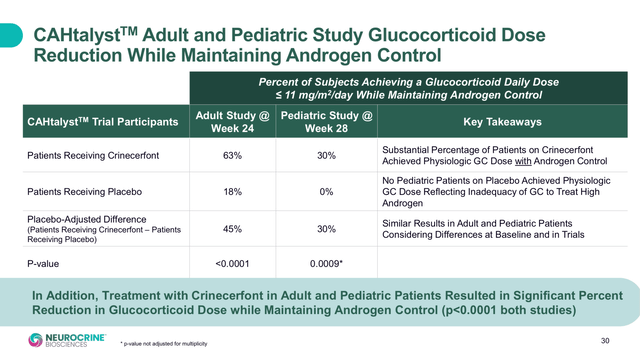
Managing classic congenital adrenal hyperplasia (CAH) in children is a delicate balancing act. For decades, the standard of care has relied on glucocorticoid replacement therapy to suppress the overproduction of adrenal androgens. While effective at controlling androgen levels, these medications often come with a significant cost: stunted growth, metabolic complications, and a higher risk of obesity.
The emergence of crinecerfont, a selective CRH receptor 1 antagonist, offers a new pathway for managing this condition. By targeting the root of the hormonal imbalance at the pituitary level, this therapy aims to lower androgen production while allowing clinicians to reduce the overall dose of glucocorticoids. This shift could fundamentally improve the long-term health and development of children living with classic CAH.
Understanding the Mechanism: How Crinecerfont Works
In patients with classic CAH, a deficiency in the 21-hydroxylase enzyme prevents the adrenal glands from producing sufficient cortisol. The body responds to this deficiency by increasing the production of corticotropin-releasing hormone (CRH) and adrenocorticotropic hormone (ACTH). While ACTH is intended to stimulate cortisol production, in CAH patients, it instead drives the overproduction of adrenal androgens.
Crinecerfont works as a CRH receptor 1 antagonist. It blocks the action of CRH at the pituitary gland, which directly reduces the secretion of ACTH. By lowering ACTH levels, the drive to produce excess androgens is diminished. This mechanism provides a “steroid-sparing” effect, meaning the patient may achieve hormonal balance with lower doses of exogenous glucocorticoids than previously required.
The Glucocorticoid Dilemma in Pediatric Patients
For children, the stakes of glucocorticoid dosing are exceptionally high. The therapeutic window is narrow, and the consequences of mismanaged dosing are severe:
- Over-treatment: Excessive glucocorticoids can lead to growth failure, premature closure of epiphyseal plates, and increased risk of insulin resistance.
- Under-treatment: Insufficient glucocorticoid levels leave children vulnerable to adrenal crises—life-threatening emergencies characterized by severe hypotension, dehydration, and shock.
The primary goal of incorporating a therapy like crinecerfont is to move the patient toward a more physiologic dose of glucocorticoids—providing enough to maintain basic health and prevent crisis, but not so much that it impairs natural growth and development.
Clinical Strategies for Safe Glucocorticoid Reduction
Reducing glucocorticoid exposure is not a process that can be rushed. Expert clinical perspectives emphasize a cautious, highly monitored approach to avoid triggering adrenal insufficiency. Key strategies include:
Gradual Tapering
Glucocorticoid doses must be reduced incrementally. A slow taper allows the body to adjust and enables clinicians to identify the minimum effective dose required to maintain stability.
Establishing a Physiologic Floor
Reduction should never proceed below the dose necessary to provide physiologic cortisol replacement. The goal is not to eliminate glucocorticoids entirely—as CAH patients still require them for survival—but to eliminate the “supraphysiologic” doses previously used solely for androgen suppression.
Frequent Monitoring
Close surveillance is mandatory during the reduction phase. This includes regular monitoring of androgen levels and clinical assessments of growth, weight, and overall well-being to ensure that the reduction in steroids isn’t compromising the patient’s health.
- Targeted Action: Crinecerfont reduces ACTH levels by blocking CRH receptors, which in turn lowers adrenal androgens.
- Growth Preservation: The primary benefit of reducing glucocorticoids is the potential for improved linear growth and fewer metabolic side effects.
- Safety First: Steroid reduction must be gradual and monitored by an endocrinologist to prevent adrenal crisis.
- Physiologic Goals: The objective is to maintain the minimum necessary steroid dose for health while utilizing crinecerfont for androgen control.
Frequently Asked Questions
Can crinecerfont completely replace glucocorticoids?
No. Because classic CAH involves a fundamental inability to produce cortisol, glucocorticoid replacement remains a lifelong necessity to prevent adrenal crisis. Crinecerfont is designed to reduce the amount of steroids needed, not replace them entirely.
How soon can we expect to see growth improvements?
Growth improvements are typically gradual. As glucocorticoid doses are lowered to more physiologic levels, the inhibitory effect on the growth plates is reduced, allowing for a more natural growth trajectory over time.

What are the signs that a steroid dose is being reduced too quickly?
Caregivers should watch for signs of adrenal insufficiency, including extreme fatigue, nausea, vomiting, abdominal pain, or unexplained irritability. Any of these symptoms require immediate medical attention.
Conclusion
The integration of CRH receptor 1 antagonists into the treatment of pediatric classic CAH represents a significant shift toward personalized, precision medicine. By decoupling androgen suppression from cortisol replacement, clinicians can better protect the growth and development of children while maintaining endocrine stability. As more practical guidelines for glucocorticoid reduction emerge, the focus remains on a patient-centered approach that prioritizes safety and long-term quality of life.
Related reading