{kind=link}
Advancements in Deep Brain Stimulation: From Invasive Surgery to Targeted Noninvasive Therapies
Deep brain stimulation (DBS) is evolving from a strictly invasive surgical procedure into more precise, and potentially noninvasive, neurological interventions. Recent research, including mouse models exploring multi-electrode configurations and clinical trials testing noninvasive stimulation, suggests a shift toward reducing the physical risks associated with traditional electrode implantation for conditions like Parkinson’s disease.
How does the new multi-electrode approach improve DBS precision?
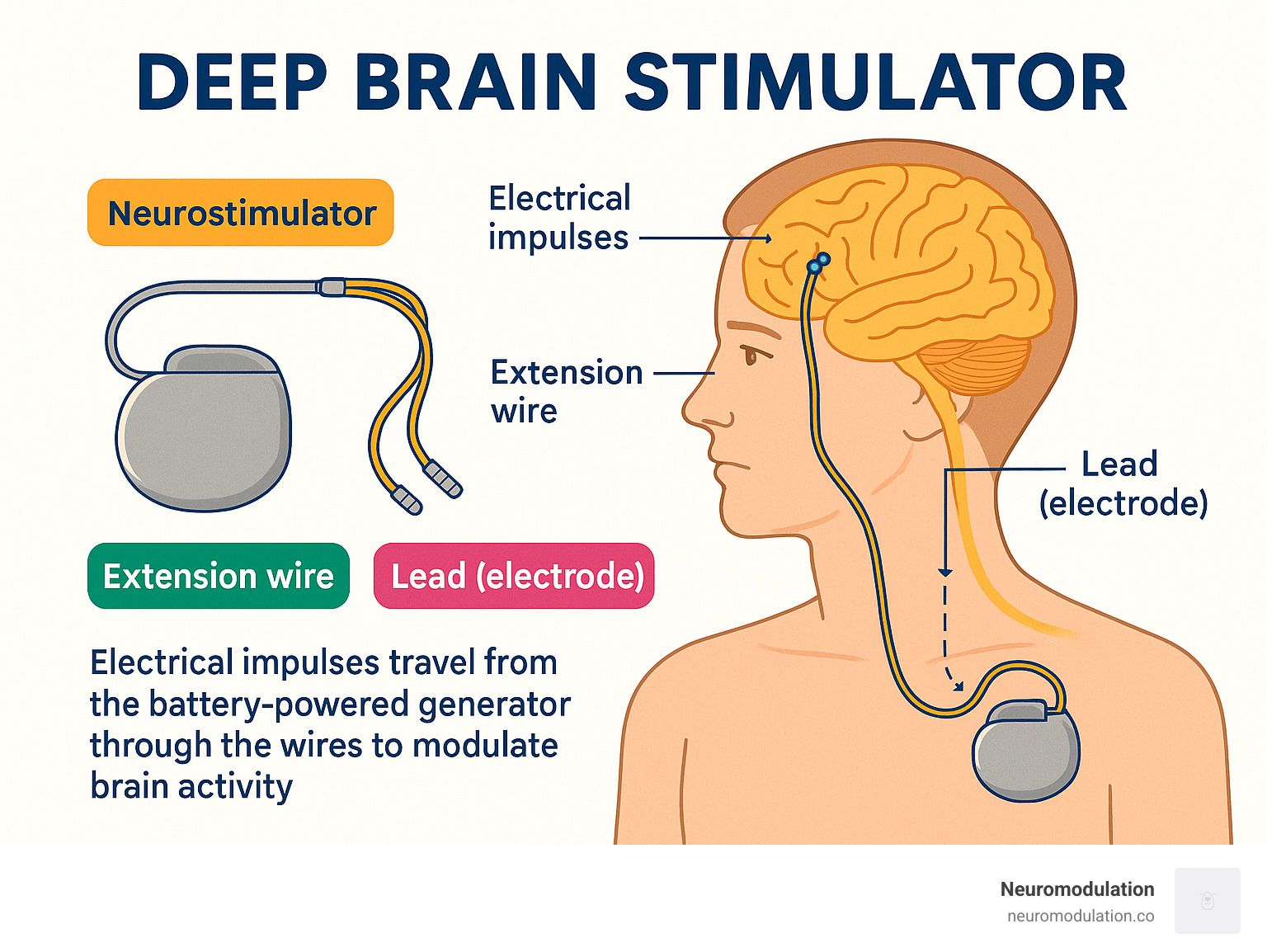
Traditional DBS involves implanting electrodes into specific brain regions to deliver electrical pulses that manage motor symptoms. A study published in Nature Communications indicates that using a third pair of electrodes can significantly sharpen the focus of these pulses. Researchers found that this configuration allows for more precise control over the electrical field, effectively isolating targeted neural circuits while sparing surrounding healthy tissue. By minimizing the spread of stimulation to unintended areas, this method may reduce the side effects often associated with conventional, broader-field stimulation techniques.

Can deep brain stimulation be performed without surgery?
Noninvasive brain stimulation is moving from experimental models to clinical testing. A recent trial published in Nature Medicine demonstrated that specialized noninvasive techniques could reduce motor symptoms in patients with Parkinson’s disease. Unlike traditional DBS, which requires a neurosurgeon to drill into the skull and place permanent leads, these noninvasive methods use external devices—such as magnetic or transcranial electrical stimulators—to influence neural activity through the scalp. According to the research, this approach offers a path to symptom management without the infection risks, hardware maintenance, or physical trauma inherent in invasive neurosurgery.
How do invasive and noninvasive methods compare?
| Feature | Invasive DBS (Traditional) | Noninvasive Stimulation |
|---|---|---|
| Procedure | Surgical implantation of leads | External device/electrodes |
| Precision | High (Direct neural access) | Moderate (Depth penetration challenges) |
| Risk Profile | Infection, hemorrhage, hardware failure | Minimal (Skin irritation, mild headache) |
| Current Status | Standard of care for advanced cases | Emerging clinical trials |
What challenges remain for noninvasive techniques?
While the prospect of noninvasive treatment is promising, medical experts highlight significant technical hurdles. According to findings from the Healthcare in Europe reporting on neuro-modulation, the primary challenge remains signal depth and intensity. The human skull acts as a barrier that dissipates electrical energy, making it difficult to target deep-seated structures like the subthalamic nucleus with the same intensity as an implanted electrode. While mouse experiments show success in focused, noninvasive delivery, translating this efficacy to human anatomy requires overcoming the physical attenuation of energy as it passes through bone and tissue.
Key considerations for patients
- Surgical Necessity: Invasive DBS remains the gold standard for patients with advanced Parkinson’s who do not respond to medication.
- Research Phase: Most noninvasive options currently discussed in clinical literature are still in the trial phase and are not yet broadly available as a replacement for surgery.
- Consultation: Patients should discuss treatment options exclusively with movement disorder specialists or neurosurgeons who have access to the latest clinical data.
The field is currently balancing the high efficacy of invasive hardware with the low-risk profile of emerging noninvasive technology. As research continues to improve the focal precision of both methods, the goal remains the same: providing patients with consistent, long-term symptom relief with the fewest possible complications.