{kind=link}
Faster-Acting Insulin Analogues vs. Human Insulin for Type 1 Diabetes: Clinical Evidence
Recent clinical evidence suggests that five faster-acting insulin analogues offer comparable glycemic control to regular human insulin for individuals with type 1 diabetes. While these analogues—including insulin lispro, insulin aspart, and ultra-rapid lispro—may reduce the incidence of severe hypoglycemic events, current data remains limited regarding long-term outcomes and quality of life improvements. These findings are based on a systematic review updated as of May 2025, which evaluated 6,335 participants across 15 randomized controlled trials.
How Do Faster-Acting Analogues Differ from Regular Insulin?
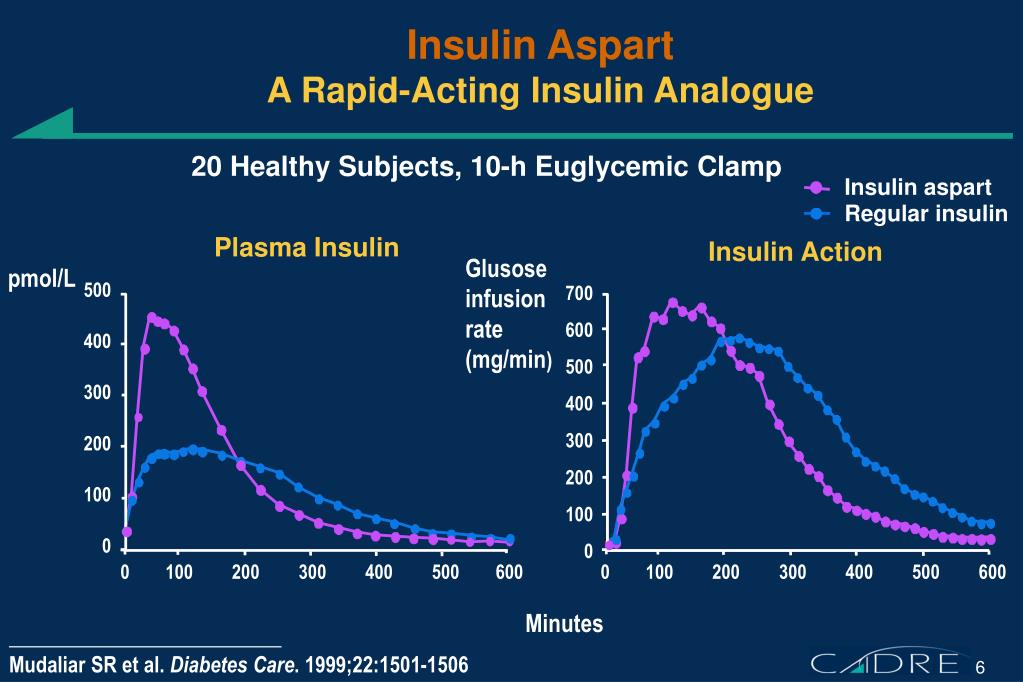
Regular human insulin requires a lead time before it begins to lower blood glucose, often necessitating injection 30 minutes before a meal. According to the American Diabetes Association (ADA), faster-acting analogues are molecularly modified to be absorbed more rapidly from the subcutaneous tissue. These agents, which include insulin aspart, insulin glulisine, and newer formulations like ultra-rapid lispro (URLi) and fast-acting aspart (FIAsp), allow patients to inject immediately before or even after starting a meal. This pharmacokinetic profile is designed to better mimic the natural insulin response of a healthy pancreas following carbohydrate intake.

Impact on Blood Glucose Control and Hypoglycemia
Clinical trials indicate that faster-acting analogues perform similarly to human insulin regarding short-term HbA1c levels, the primary marker for long-term blood sugar management. However, the safety profile shows distinct differences. Data analyzed by researchers suggests that these analogues may be associated with a lower risk of severe hypoglycemia—episodes where blood glucose drops to levels requiring third-party assistance. According to the Cochrane Library, while the evidence points toward a reduction in severe hypoglycemic episodes, the clinical certainty regarding nocturnal (nighttime) hypoglycemia remains low due to inconsistencies in study reporting and participant monitoring.
Limitations of Current Clinical Evidence
Despite the widespread use of these analogues, the strength of the existing evidence is constrained by several factors. Most of the 15 studies included in recent systematic reviews were conducted in an unblinded fashion, meaning both researchers and participants were aware of the treatment being administered. This design introduces a risk of bias. Furthermore, the studies typically monitored participants for periods between 24 and 52 weeks. There is a notable lack of long-term data—defined as follow-up periods exceeding one year—which limits our understanding of the sustained impact of these medications on chronic diabetes complications.
Key Comparison: Faster-Acting Analogues vs. Regular Insulin
| Outcome | Comparison Result |
|---|---|
| HbA1c Levels (Short-term) | Similar effectiveness |
| Severe Hypoglycemia | Potential reduction with analogues |
| Nocturnal Hypoglycemia | Evidence unclear |
| Quality of Life | No clear evidence of difference |
What Patients Should Consider
Choosing between insulin types is a clinical decision that should be made in consultation with an endocrinologist or a certified diabetes care and education specialist. While faster-acting analogues provide increased flexibility for mealtime dosing, they do not replace the need for consistent blood glucose monitoring. Patients should discuss their specific glycemic patterns, lifestyle requirements, and insurance coverage with their healthcare provider. As of 2025, the National Institute of Diabetes and Digestive and Kidney Diseases continues to emphasize that adherence to a prescribed insulin regimen remains the most critical factor in preventing diabetic ketoacidosis and other acute complications, regardless of the specific type of insulin used.
