{kind=link}
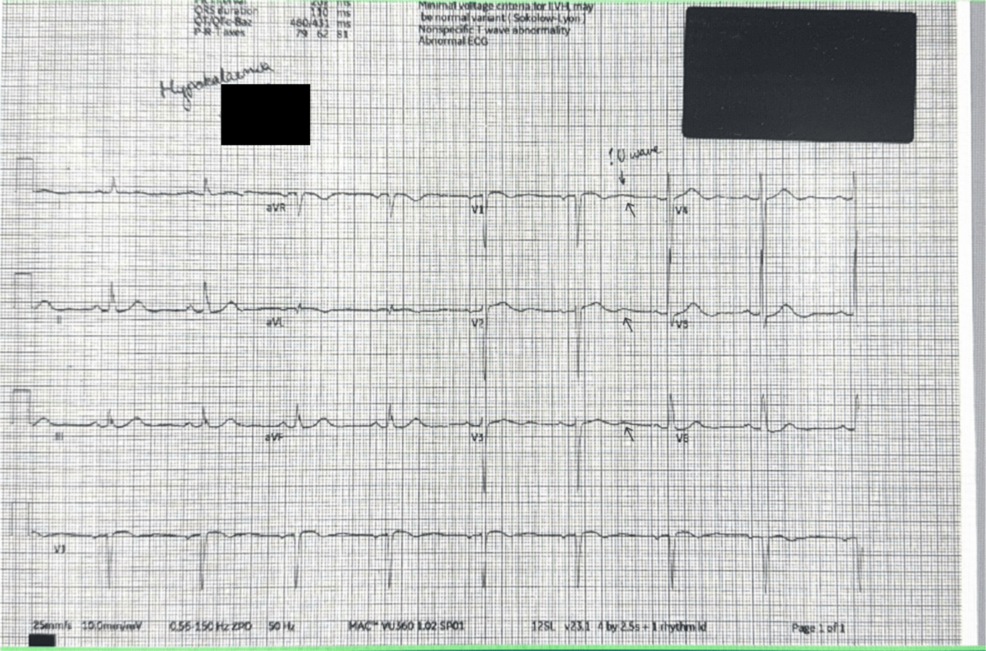
Fludrocortisone can cause hypokalaemia, a dangerous drop in blood potassium levels, particularly in older adults. This mineralocorticoid medication works by retaining sodium and excreting potassium through the kidneys. When potassium levels fall too low, patients risk cardiac arrhythmias, muscle weakness, and severe metabolic imbalances, according to the National Library of Medicine.
What is Fludrocortisone and how does it work?
Fludrocortisone is a synthetic steroid used primarily to treat primary adrenal insufficiency (Addison’s disease) and orthostatic hypotension. It mimics the action of aldosterone, a hormone produced by the adrenal glands. According to the U.S. Food and Drug Administration (FDA), the drug increases the reabsorption of sodium and water in the distal renal tubules, which helps maintain blood pressure and fluid volume.
The trade-off for this sodium retention is the active secretion of potassium into the urine. This process is the primary mechanism that leads to potassium depletion, or hypokalaemia, if not closely monitored with dietary supplementation or potassium-sparing medications.
Why does fludrocortisone trigger hypokalaemia in older adults?
Older adults are more susceptible to medication-induced electrolyte imbalances due to declining kidney function and a higher likelihood of taking multiple medications (polypharmacy). The Mayo Clinic notes that age-related decreases in the glomerular filtration rate (GFR) can alter how the body processes steroids, potentially exacerbating the loss of potassium.
When fludrocortisone forces the kidneys to dump potassium to save sodium, the body’s stores deplete. If a patient is already on a low-potassium diet or taking diuretics—such as furosemide or hydrochlorothiazide—the risk of severe hypokalaemia increases significantly. This combination can lead to a “double hit” where both the steroid and the diuretic strip the body of essential minerals.
What are the symptoms of low potassium?
Hypokalaemia often starts with subtle signs that can be mistaken for general aging or other chronic conditions. Common symptoms include:
- Muscle Weakness: Difficulty climbing stairs or rising from a chair.
- Cardiac Irregularities: Heart palpitations or an irregular heartbeat (arrhythmia).
- Gastrointestinal Issues: Constipation or abdominal bloating due to slowed smooth muscle contraction.
- Neurological Effects: Severe fatigue, cramping, or in extreme cases, paralysis.
According to the Merck Manual, severe potassium deficiency can lead to rhabdomyolysis (muscle breakdown) and acute kidney injury.
How is fludrocortisone-associated hypokalaemia managed?
Management requires a balance between maintaining blood pressure and stabilizing electrolytes. Physicians typically employ three primary strategies:

1. Dosage Adjustment: Reducing the fludrocortisone dose to the minimum effective level to limit potassium excretion.
2. Potassium Supplementation: Introducing oral potassium chloride or encouraging a diet rich in potassium, such as bananas, spinach, and potatoes.
3. Co-administration of Potassium-Sparing Diuretics: In some cases, doctors prescribe medications like spironolactone, which blocks the effect of aldosterone (and fludrocortisone) on potassium excretion in the kidneys.
Comparing Potassium Risks: Fludrocortisone vs. Other Steroids
| Medication Type | Primary Action | Potassium Impact | Common Use Case |
|---|---|---|---|
| Fludrocortisone | Strong Mineralocorticoid | High risk of excretion (Loss) | Orthostatic Hypotension |
| Prednisone | Strong Glucocorticoid | Mild to Moderate risk | Inflammation/Autoimmune |
| Hydrocortisone | Mixed Action | Moderate risk | Adrenal Insufficiency |
Frequently Asked Questions
Can I take potassium supplements while on fludrocortisone?
Yes, but only under medical supervision. Over-supplementing can lead to hyperkalaemia (too much potassium), which is equally dangerous for the heart. Regular blood tests are required to find the correct balance.
How often should potassium levels be checked?
According to clinical guidelines for steroid therapy, electrolyte levels should be checked shortly after starting the medication and periodically throughout treatment, especially in elderly patients or those with renal impairment.
Is this a common side effect?
While not every patient develops hypokalaemia, potassium loss is a well-documented pharmacological effect of mineralocorticoids. The risk is significantly higher in patients with pre-existing kidney issues or those using other diuretic medications.