{kind=link}
Understanding Idiopathic Avascular Necrosis of the Femoral Head in Older Adults
Idiopathic avascular necrosis (AVN) of the femoral head—also known as osteonecrosis—is a debilitating condition characterized by the death of bone tissue due to a lack of blood supply, occurring in the absence of a clear identifiable cause. While often associated with trauma or steroid use, clinical cases in older adults frequently present diagnostic challenges due to the condition’s mimicry of common age-related joint issues like osteoarthritis. According to the American Academy of Orthopaedic Surgeons (AAOS), early detection is vital, as the condition can lead to the collapse of the femoral head and permanent joint destruction if left untreated.
What Causes Idiopathic Avascular Necrosis?
The term “idiopathic” indicates that the underlying trigger for the blood supply disruption remains unknown. In many patients, however, researchers look for subtle risk factors that may contribute to the pathology. The National Institutes of Health (NIH) notes that even when a specific cause cannot be pinpointed, the mechanism involves the interruption of blood flow to the trabecular bone of the femoral head. Without oxygen and nutrients, the bone tissue begins to die, weakening the structural integrity of the hip joint.

How Does the Condition Present in Older Adults?
In older populations, symptoms of AVN are often indistinguishable from severe hip osteoarthritis, which can delay diagnosis. Patients typically report:
- Groin Pain: The most common symptom, which may radiate to the thigh or knee.
- Reduced Range of Motion: Difficulty with internal rotation or abduction of the hip.
- Weight-Bearing Discomfort: Pain that worsens significantly when walking or standing.
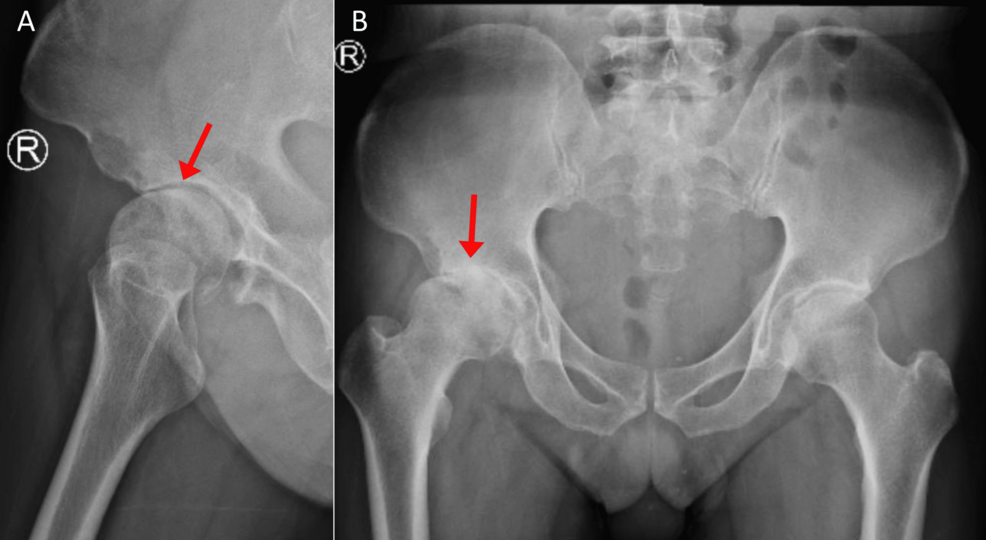
According to research published in the journal Cureus, clinicians must maintain a high index of suspicion for AVN in elderly patients who present with persistent hip pain that does not correlate with the severity of findings on initial X-rays. Because standard radiographs may appear normal in the early stages of the disease, magnetic resonance imaging (MRI) remains the gold standard for definitive diagnosis.
Diagnostic and Treatment Approaches
Diagnosis relies on advanced imaging. While X-rays can show bone collapse in later stages, an MRI can detect early-stage bone marrow edema and necrotic changes before the bone structure fails.
Treatment strategy is dictated by the stage of the necrosis. The Johns Hopkins Medicine clinical guidelines suggest two primary paths:
| Stage | Typical Intervention |
|---|---|
| Early Stage (Pre-collapse) | Core decompression, bone grafting, or vascularized bone grafts to restore blood flow. |
| Late Stage (Post-collapse) | Total hip arthroplasty (hip replacement) to restore function and alleviate pain. |
Why Early Intervention Matters
The primary concern with idiopathic AVN is the progression to femoral head collapse. Once the bone surface loses its smooth contour, the resulting friction causes rapid deterioration of the acetabulum (the hip socket), leading to secondary arthritis. According to the American College of Rheumatology, patients who receive surgical intervention before the structural collapse of the femoral head typically experience better long-term functional outcomes compared to those who require late-stage joint replacement.

Key Takeaways for Patients
- Persistent Pain: If you experience persistent, unexplained groin or hip pain, consult an orthopedic specialist immediately.
- Imaging: Do not rely solely on X-rays; ask your physician if an MRI is necessary to rule out osteonecrosis.
- Proactive Management: Early-stage intervention is significantly less invasive than total hip replacement and offers a better chance of preserving the natural joint.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions regarding a medical condition.
Keep reading