{kind=link}
Uterus Didelphys and Pregnancy: Navigating Diagnostic Challenges
Uterus didelphys, a rare congenital uterine anomaly characterized by the presence of two separate uteri and two cervices, can significantly complicate the clinical diagnosis of pregnancy. When a patient presents with abdominal pain, the anatomical complexity of a duplicate uterus often leads to the misdiagnosis of an intrauterine pregnancy as an ectopic pregnancy, potentially resulting in unnecessary surgical interventions.
Understanding Uterus Didelphys
Uterus didelphys is a Mullerian duct anomaly that occurs during fetal development when the two Mullerian ducts fail to fuse. According to the [American College of Obstetricians and Gynecologists (ACOG)](https://www.acog.org/), this results in a complete duplication of the uterine anatomy. Individuals with this condition often have two distinct uterine horns, two cervices, and sometimes a longitudinal vaginal septum.
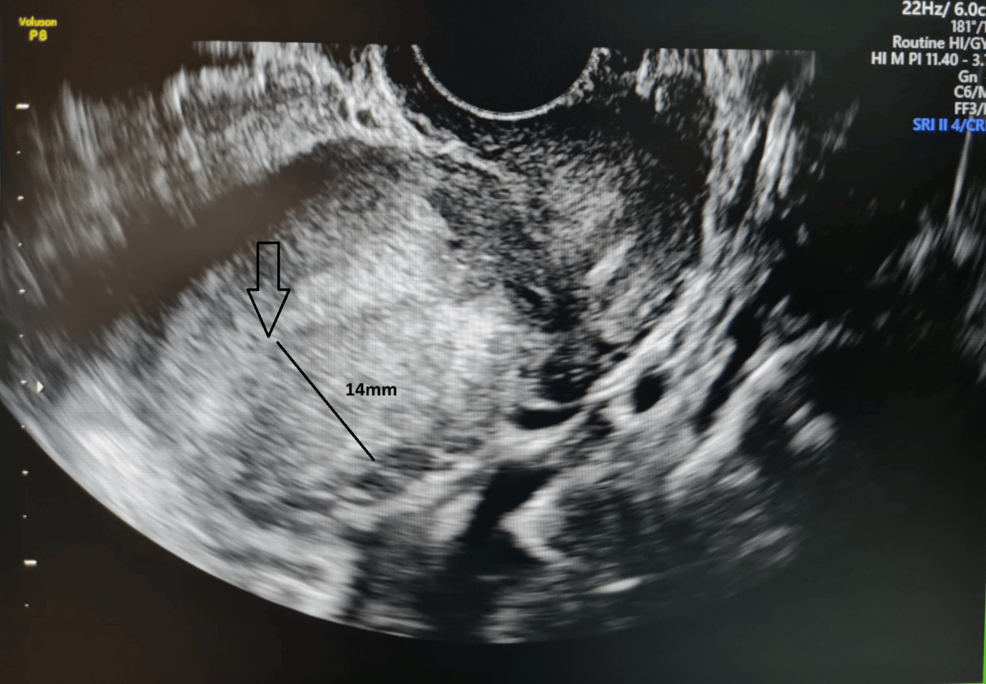
While many individuals with uterus didelphys remain asymptomatic and may have successful pregnancies, the anatomical variation can create challenges for clinicians. The primary difficulty arises during early pregnancy, when the location of the gestational sac within one of the two uterine horns can mimic the appearance of an extrauterine, or ectopic, pregnancy on ultrasound.
Diagnostic Challenges and Misinterpretation
The misdiagnosis of an intrauterine pregnancy as an ectopic pregnancy is a documented clinical concern. In patients with uterus didelphys, the empty uterine horn can be mistaken for the primary uterus, while the pregnant horn is incorrectly identified as an adnexal mass.
Diagnostic accuracy relies heavily on high-resolution imaging. The [Society of Radiologists in Ultrasound](https://www.sru.org/) emphasizes that a thorough pelvic examination combined with transvaginal ultrasound is essential for identifying the specific anatomy of the uterine cavity. When a pregnancy is identified, clinicians must confirm its location within the endometrial cavity of one of the horns to rule out a concurrent ectopic pregnancy.
Clinical Implications for Patient Care
Misidentifying a viable intrauterine pregnancy as an ectopic pregnancy carries significant risks. Ectopic pregnancies are typically managed with medical therapy, such as methotrexate, or surgical intervention. Administering methotrexate to a patient with a viable intrauterine pregnancy can lead to severe fetal complications or pregnancy loss.
To prevent diagnostic errors, clinical protocols prioritize the following:
- Detailed Anatomical Mapping: Utilizing 3D ultrasound or magnetic resonance imaging (MRI) to confirm the presence of dual uteri before proceeding with invasive procedures.
- Serial Beta-hCG Monitoring: Tracking human chorionic gonadotropin levels to assess the viability and progression of the pregnancy.
- Multidisciplinary Consultation: Engaging maternal-fetal medicine specialists when anatomical anomalies are suspected to ensure accurate diagnosis and appropriate management.
Managing Pregnancy with Uterine Anomalies
Pregnancies in patients with uterus didelphys are generally considered high-risk, though many progress to term. The [National Institutes of Health (NIH)](https://www.nichd.nih.gov/) notes that patients with uterine anomalies may face an increased risk of preterm labor, malpresentation, and intrauterine growth restriction.
Because the uterus is divided, the available space for the fetus may be reduced compared to a typical uterus. Regular prenatal surveillance, including frequent growth scans, is standard practice to monitor fetal development and maternal health.
Key Takeaways for Patients and Providers
- Uterus didelphys is a rare congenital condition that requires specialized imaging to differentiate from other gynecological or obstetric conditions.
- Early ultrasound findings in patients with duplicate uteri can be misleading; clinicians must verify the location of the gestational sac within the uterine cavity.
- Avoiding unnecessary medical or surgical intervention is critical when a viable pregnancy is identified in one of the two uterine horns.
- Patients diagnosed with uterus didelphys should be managed by obstetricians experienced in handling uterine anomalies to optimize pregnancy outcomes.
As diagnostic technology advances, the ability to accurately identify and manage pregnancies in patients with complex uterine anatomy continues to improve, reducing the incidence of misdiagnosis and ensuring safer care for both mother and fetus.
Worth a look