{kind=link}
Kounis syndrome is a clinical condition defined by the concurrence of acute coronary syndrome with conditions associated with mast cell activation, such as allergic, hypersensitivity, or anaphylactic reactions. First described by Dr. Nicholas Kounis in 1991, the syndrome involves the release of inflammatory mediators—including histamine, neutral proteases, and arachidonic acid products—that trigger coronary artery spasm or plaque erosion, according to the Journal of the American College of Cardiology.
How Does Kounis Syndrome Develop?
The pathophysiology of Kounis syndrome centers on the activation of mast cells within the coronary arterial wall or systemic circulation. When these cells degranulate in response to an allergen, they release substances that directly affect the heart. Research published in the European Heart Journal identifies three distinct variants of the syndrome:

- Type I: Occurs in patients with normal coronary arteries who experience coronary spasm, potentially leading to myocardial infarction.
- Type II: Occurs in patients with pre-existing coronary artery disease where an allergic insult induces plaque rupture or erosion.
- Type III: Involves stent thrombosis, where inflammatory mediators triggered by an allergic reaction promote the formation of a thrombus within a previously implanted drug-eluting stent.
What Are the Common Triggers?
Kounis syndrome can be triggered by a wide array of environmental and medical exposures. Because the underlying mechanism is an allergic response, any substance capable of inducing systemic mast cell activation is a potential candidate. According to the Texas Heart Institute, common triggers include:

- Medications: Antibiotics (such as penicillins and cephalosporins), nonsteroidal anti-inflammatory drugs (NSAIDs), and contrast media used in imaging.
- Environmental Factors: Bee or wasp stings and exposure to certain plants.
- Foods and Additives: Shellfish, nuts, or preservatives in processed foods.
- Medical Devices: Materials used in stents or surgical implants.
How Is the Condition Diagnosed and Managed?
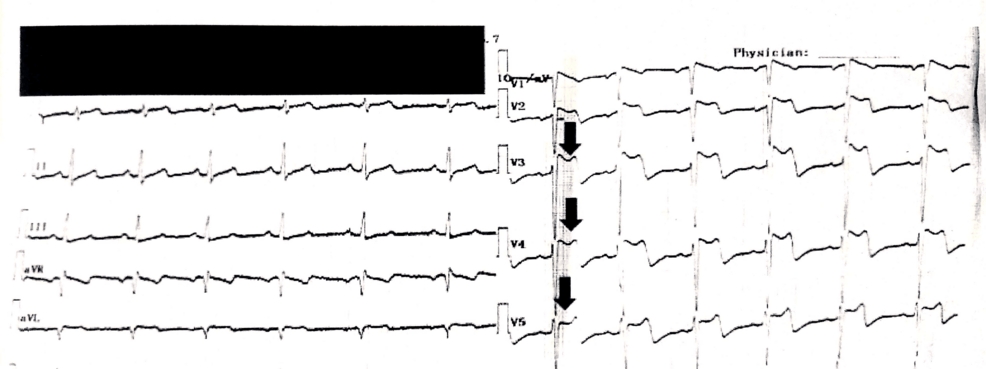
Diagnosing Kounis syndrome requires a high index of suspicion because the symptoms of an allergic reaction—such as hives, wheezing, or hypotension—can distract from the concurrent cardiac event. Clinicians must perform an electrocardiogram (ECG) and monitor cardiac biomarkers like troponin in any patient presenting with an acute allergic reaction who also reports chest pain, according to the National Institutes of Health (NIH).

Treatment is complex because standard protocols for myocardial infarction and anaphylaxis may sometimes conflict. For example, epinephrine is the first-line treatment for anaphylaxis but can exacerbate coronary spasm in Kounis syndrome patients. Therefore, management often requires a delicate balance of antihistamines, corticosteroids, and cautious use of vasodilators to address both the allergic inflammatory cascade and the compromised coronary blood flow.
Is Kounis Syndrome Underrecognized?
Medical literature consistently characterizes Kounis syndrome as an underrecognized cause of acute coronary events. Because the cardiac symptoms may be overshadowed by the visible signs of allergy, or conversely, because the allergic reaction may be mild or overlooked, the diagnosis is frequently missed in emergency settings. Increased awareness among healthcare providers regarding the link between mast cell activation and coronary artery physiology is essential for improving patient outcomes and preventing misdiagnosis in acute care settings.