{kind=link}
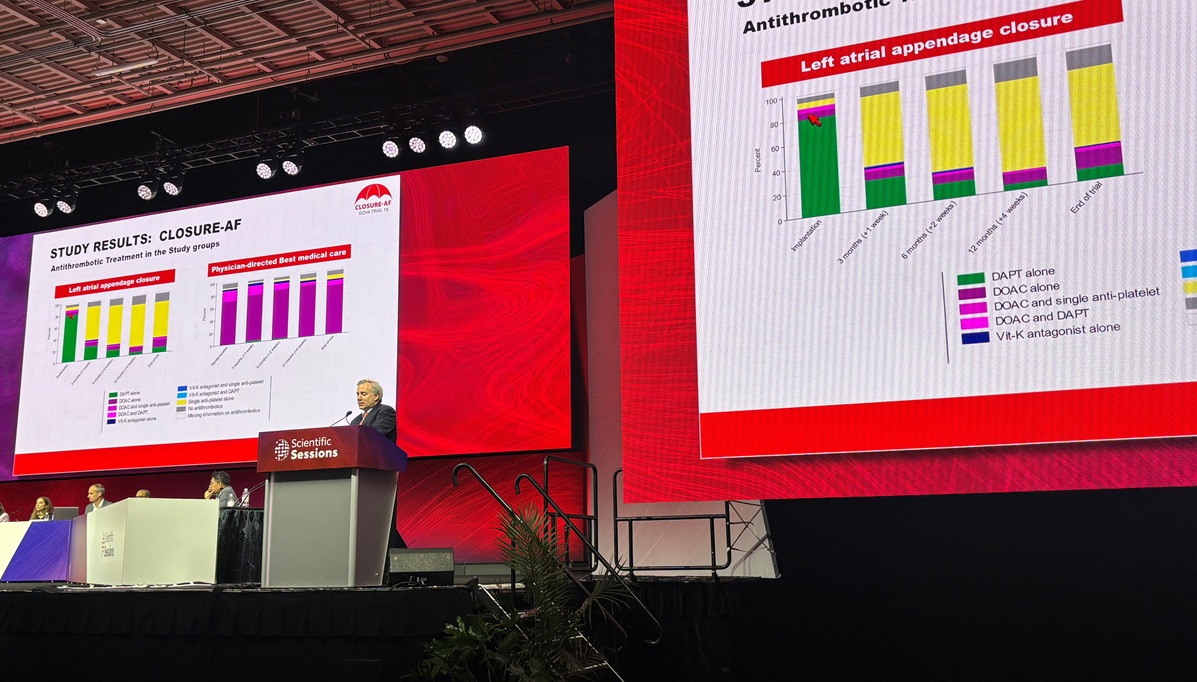
LAAO vs. Medical Therapy for Atrial Fibrillation: CLOSURE-AF Trial Results
For patients with atrial fibrillation (AF) at high risk of both stroke and bleeding, left atrial appendage occlusion (LAAO) is not superior to standard medical care, including anticoagulants, according to findings from the CLOSURE-AF trial. The results, presented at the American Heart Association (AHA) 2025 Scientific Sessions and subsequently published in the Modern England Journal of Medicine, challenge previous assumptions about the role of LAAO in this high-risk population.
Understanding the CLOSURE-AF Trial
The CLOSURE-AF trial was a randomized (1:1) study comparing percutaneous LAAO with optimized medical therapy in 912 patients with AF who were at high risk for both stroke (CHA₂DS₂-VASc score ≥ 2) and bleeding (HAS-BLED score ≥ 3, prior major or intracranial bleeding, or chronic kidney disease). The majority of patients in the medical therapy arm received direct oral anticoagulants (DOACs). Participants were followed for a median of 3 years.
The primary endpoint was a composite of stroke (ischemic or hemorrhagic), systemic embolism, cardiovascular or unexplained death, or major bleeding (BARC ≥ 3).
Key Findings: Medical Therapy Outperforms LAAO
The trial found that LAAO did not meet the criteria for non-inferiority compared to medical therapy (P for noninferiority = 0.44). In fact, the LAAO group experienced a higher risk of the composite primary endpoint, with an adjusted hazard ratio of 1.28 (95% CI 1.01-1.62) favoring standard medical care. This difference was primarily driven by an increase in embolic events.
The incidence of the primary endpoint was 16.83 per 100 person-years in the LAAO group and 13.27 per 100 person-years in the medical therapy group. Individual components of the composite endpoint occurred at similar rates, but the study was not powered to detect differences in these specific outcomes.
Expert Perspectives and Implications
Dr. Ulf Landmesser, who presented the trial at AHA 2025, acknowledged that the results were unexpected, particularly given the increasing use of LAAO in this patient population. He indicated he would likely modify his practice based on the CLOSURE-AF findings, suggesting that patients at high risk may not be optimal candidates for the procedure. NEJM
Jeff Healey, MD, the discussant for CLOSURE-AF, highlighted that while LAAO is widely used due to concerns about oral anticoagulant discontinuation, there has been limited randomized controlled trial (RCT) data to guide practice, especially in patients with a history of bleeding. ACC
Andrew Goldsweig, MD, noted that the trial results should be interpreted in the context of evolving LAAO techniques and devices. He suggested that trials conducted with current devices may yield different results. He emphasized the importance of carefully balancing the risks and benefits of LAAO for each individual patient. Medscape
Future Research
Further research is ongoing to evaluate LAAO in different risk profiles. Trials such as CHAMPION-AF, CATALYST, and LAAOS-4 are investigating the role of LAAO in lower-risk and very-high-risk populations, respectively. SOLACI
Left atrial appendage closure is a mechanical alternative to anticoagulation, but data regarding its use after atrial fibrillation ablation are lacking. NEJM
Worth a look