{kind=link}
Managing ADHD Medication Shortages: Clinical Insights on Switching to Immediate-Release Dextroamphetamine
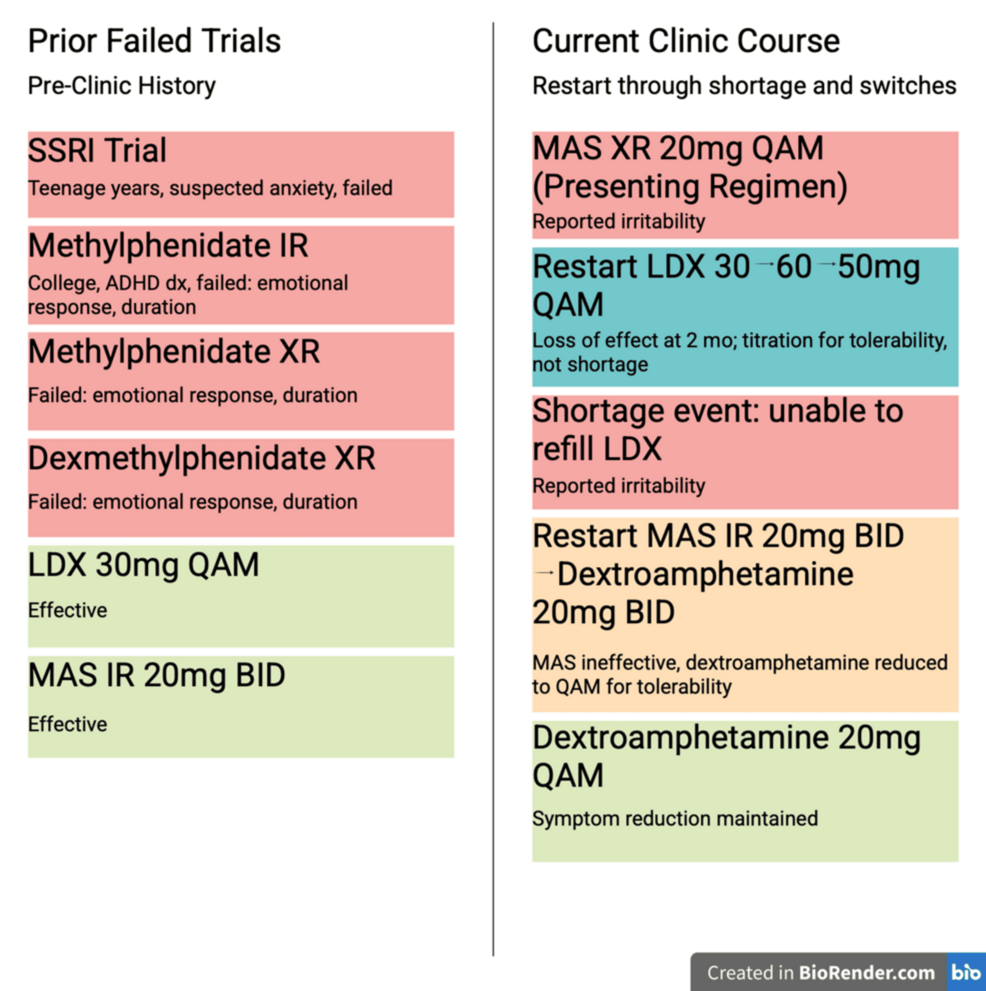
Patients experiencing persistent ADHD medication shortages can often maintain symptom control by transitioning from extended-release formulations to immediate-release (IR) dextroamphetamine. While drug shortages have disrupted treatment plans for millions, clinical evidence suggests that a carefully managed switch to IR stimulants remains a viable strategy for maintaining therapeutic efficacy when long-acting options are unavailable. This approach requires frequent dosing adjustments to account for the shorter duration of action compared to once-daily extended-release medications.
Why Stimulant Shortages Impact ADHD Treatment
The U.S. Food and Drug Administration (FDA) has reported intermittent shortages of various ADHD medications, including mixed amphetamine salts (Adderall) and methylphenidate, since 2022. These shortages stem from a combination of increased demand, manufacturing delays, and supply chain constraints. According to the Drug Enforcement Administration (DEA), which sets production quotas for controlled substances, these medications are classified as Schedule II drugs, meaning supply cannot be easily scaled to meet sudden spikes in demand.
For patients, this creates significant clinical hurdles. Extended-release formulations are often preferred for their ability to provide consistent symptom coverage throughout the school or workday. When these are unavailable, clinicians must work with patients to identify alternatives that prevent treatment gaps, which can lead to a resurgence of ADHD symptoms like inattention, impulsivity, and executive dysfunction.
Clinical Considerations for Switching to Immediate-Release Formulations
When long-acting stimulants are unavailable, the transition to immediate-release dextroamphetamine requires a specific clinical strategy. Because IR tablets typically last only three to four hours, patients must take multiple doses throughout the day to achieve the same coverage once provided by a single extended-release pill.

According to clinical guidance published in the journal Cureus, successful management relies on:
- Dosing Frequency: Patients often require two to three doses daily to mimic the 8- to 12-hour coverage of long-acting stimulants.
- Titration: Physicians must carefully calculate the total daily milligram equivalent to avoid over- or under-medicating during the transition.
- Patient Monitoring: Increased frequency of office visits or telehealth check-ins is necessary to ensure the patient tolerates the dosing schedule and that the “peaks and valleys” of IR stimulants do not cause adverse side effects like irritability or rebound symptoms.
Comparing Extended-Release vs. Immediate-Release Stimulants
The choice between these formulations involves trade-offs regarding convenience and symptom stability. The following table highlights the primary differences clinicians consider when navigating shortages.
| Feature | Extended-Release (XR/ER) | Immediate-Release (IR) |
|---|---|---|
| Dosing Schedule | Once daily | Multiple times daily |
| Symptom Control | Consistent, smooth delivery | Fluctuating (peaks and troughs) |
| Risk of Missed Doses | Low | Higher (requires adherence to schedule) |
What Happens Next for Patients
Patients struggling to fill prescriptions should communicate directly with their prescribing physician rather than attempting to source medications from multiple pharmacies, which can complicate controlled substance monitoring. The Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD) organization advises that patients ask their doctors about alternative formulations or generic versions that may have better availability in their local area.
Moving forward, the medical community continues to advocate for better supply chain transparency. While switching to immediate-release dextroamphetamine is a proven stopgap, it is considered a temporary solution until national production quotas and manufacturing capacities align more closely with the diagnostic prevalence of ADHD. Patients should prioritize maintaining a consistent relationship with their pharmacy and provider to ensure that any necessary changes to their medication regimen are documented and monitored for safety.