{kind=link}
Understanding the Medical Frailty Exemption in Medicaid Work Requirements
As federal policy shifts toward implementing work requirements for specific Medicaid populations, the “medically frail” exemption has become a focal point for both state administrators and healthcare advocates. Beginning January 1, 2027, states are required to tie Medicaid eligibility for certain adult groups—specifically those in the Affordable Care Act (ACA) expansion category—to work or community engagement activities. Protecting vulnerable patients from these mandates is a priority, and the medical frailty exemption serves as a critical safety net.
What Constitutes Medical Frailty?
The federal framework for medical frailty is designed to ensure that individuals with significant health needs are not forced into the workforce when their physical or mental health status precludes it. Under current guidelines, the definition of “medically frail” typically encompasses:
- Individuals who are blind or living with a permanent disability.
- Those with physical, intellectual, or developmental disabilities that impair their ability to perform activities of daily living (ADLs).
- Individuals with severe substance use disorders or disabling mental health conditions.
- Patients with complex, chronic, or serious medical conditions that require ongoing clinical management.
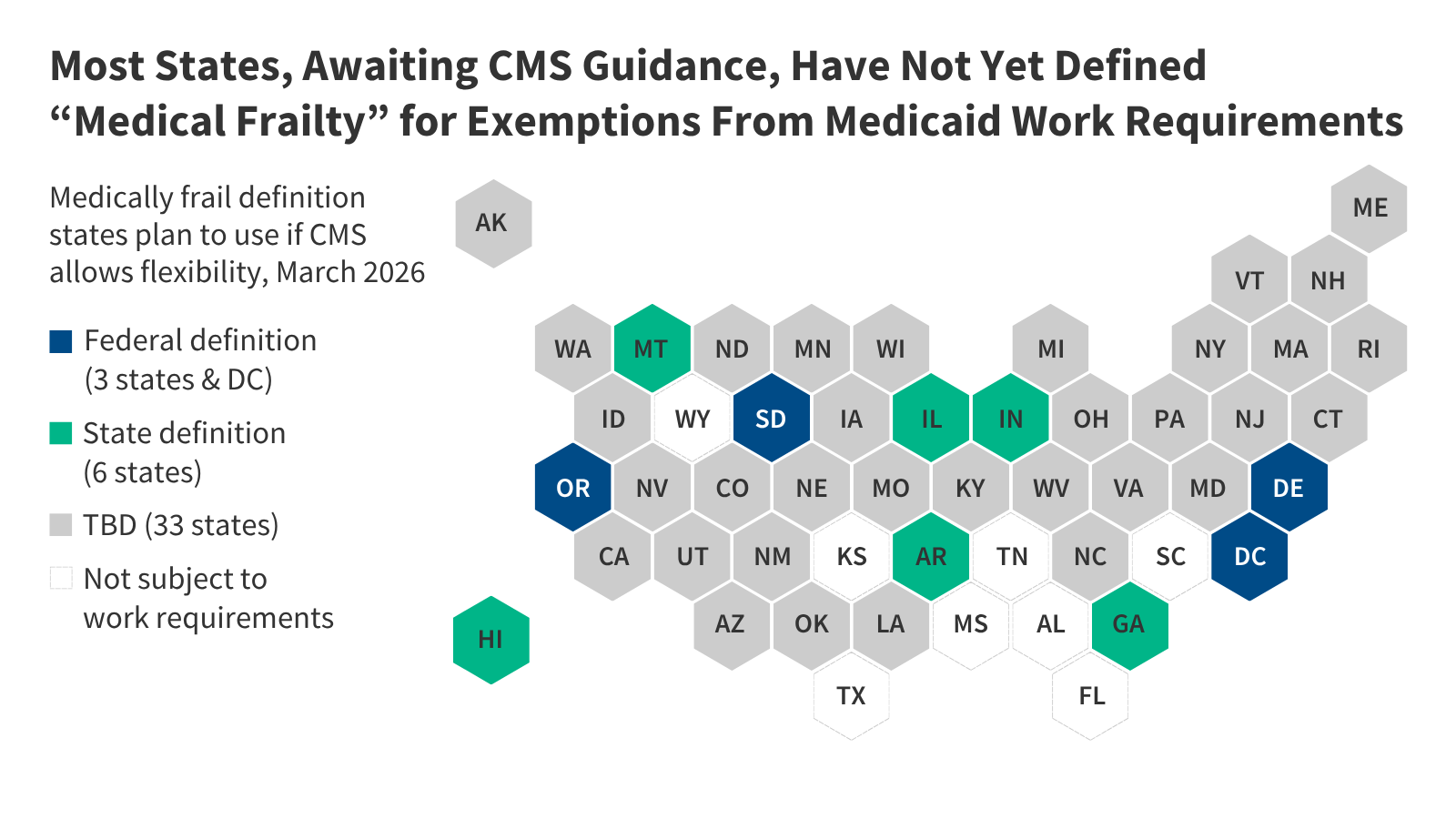
Because the interpretation of “complex medical conditions” can vary, the Centers for Medicare & Medicaid Services (CMS) is expected to release an interim final rule by June 1, 2026. This guidance aims to standardize how states identify these individuals and ensure that the exemption is applied consistently across the country.
How States Are Preparing for Implementation
State Medicaid agencies are currently in a transition period, balancing the need to build administrative infrastructure with the uncertainty of forthcoming federal regulations. While some states have existing definitions of medical frailty used for “alternative benefit plans,” these definitions often need to be modernized to meet the specific requirements of the new work mandates.

Data-Driven Verification
Most states are moving toward an automated approach to reduce the administrative burden on patients. By analyzing Medicaid claims data, states can identify enrollees with established diagnoses—such as cancer, HIV, or heart disease—that qualify them for an exemption. However, claims data has limitations. It may not reflect the health status of new applicants, and inconsistent medical coding can lead to gaps in identification.
Alternative Verification Methods
To supplement claims data, states are exploring several secondary verification strategies:
- Managed Care Data: Utilizing information from care management systems and behavioral health programs to verify health status.
- Health Screeners: Implementing standardized clinical assessments at the time of application or renewal.
- Provider Attestation: Partnering with treating physicians to confirm a patient’s inability to meet work requirements due to their health status.
Key Challenges and Considerations
The road to implementation is not without hurdles. States and federal regulators are currently grappling with how to balance administrative efficiency with patient privacy and access to care.
The Role of Self-Attestation
One of the most debated issues is whether to allow individuals to “self-attest” to their medical frailty. While this reduces the paperwork burden on patients and providers, some states have expressed concerns regarding program integrity and have moved to restrict or prohibit self-attestation entirely. CMS guidance will likely clarify whether self-attestation is an acceptable pathway and what, if any, supplemental documentation will be required.
The “Look-Back” Period
The time frame used to review an individual’s medical history—the “look-back” period—is critical. A short window may fail to capture patients with episodic conditions or those who have recently experienced a lapse in care. States are currently waiting for federal clarity on whether different look-back standards will apply to initial applications versus annual renewals.
Key Takeaways for Patients and Providers
- Safety Net Protections: The medical frailty exemption is a mandatory federal requirement, not an optional state feature. It is intended to protect those with significant health barriers.
- Importance of Accurate Coding: For providers, accurate and consistent diagnostic coding is more crucial than ever. It ensures that patients are automatically identified for exemptions without needing to navigate complex appeals processes.
- Stay Informed: As CMS releases the interim final rule in June 2026, state-specific policies will likely evolve. Patients should monitor their state’s Medicaid portal for updates regarding renewal requirements and exemption status.
the goal of the medical frailty exemption is to ensure that the pursuit of employment does not come at the expense of health. By leveraging existing clinical data and establishing clear, empathetic verification processes, states can ensure that the most vulnerable members of the Medicaid population remain covered and supported.
Disclaimer: This article is for informational purposes only and does not constitute legal or medical advice. Please consult your local Medicaid office or a qualified healthcare professional regarding your specific eligibility and health needs.