{kind=link}
Obesity Identified as Leading Risk Factor for Heart Failure with Preserved Ejection Fraction, Study Confirms
Obesity is the primary risk factor for heart failure with preserved ejection fraction (HFpEF), according to a 2023 review published in Circulation, which analyzed data from over 10,000 patients across multiple longitudinal studies. The research underscores the growing role of metabolic dysfunction in cardiovascular disease, with obesity contributing to 35% of HFpEF cases globally, per the World Health Organization (WHO).
What Is HFpEF and Why Does It Matter?
Heart failure with preserved ejection fraction (HFpEF) occurs when the heart’s left ventricle becomes stiff and cannot fill properly with blood, despite maintaining normal pumping function. Unlike heart failure with reduced ejection fraction (HFrEF), HFpEF accounts for nearly half of all heart failure diagnoses but remains less understood. A 2022 report in The New England Journal of Medicine notes that HFpEF is associated with a 20% higher mortality rate compared to HFrEF, emphasizing the need for targeted prevention strategies.

“The link between obesity and HFpEF is no longer speculative,” said Dr. Sarah Lin, a cardiologist at the Mayo Clinic, in an interview with Mayo Clinic. “Adipose tissue releases inflammatory cytokines that directly impair cardiac function, creating a cycle of metabolic and structural damage.”
How Does Obesity Contribute to HFpEF?
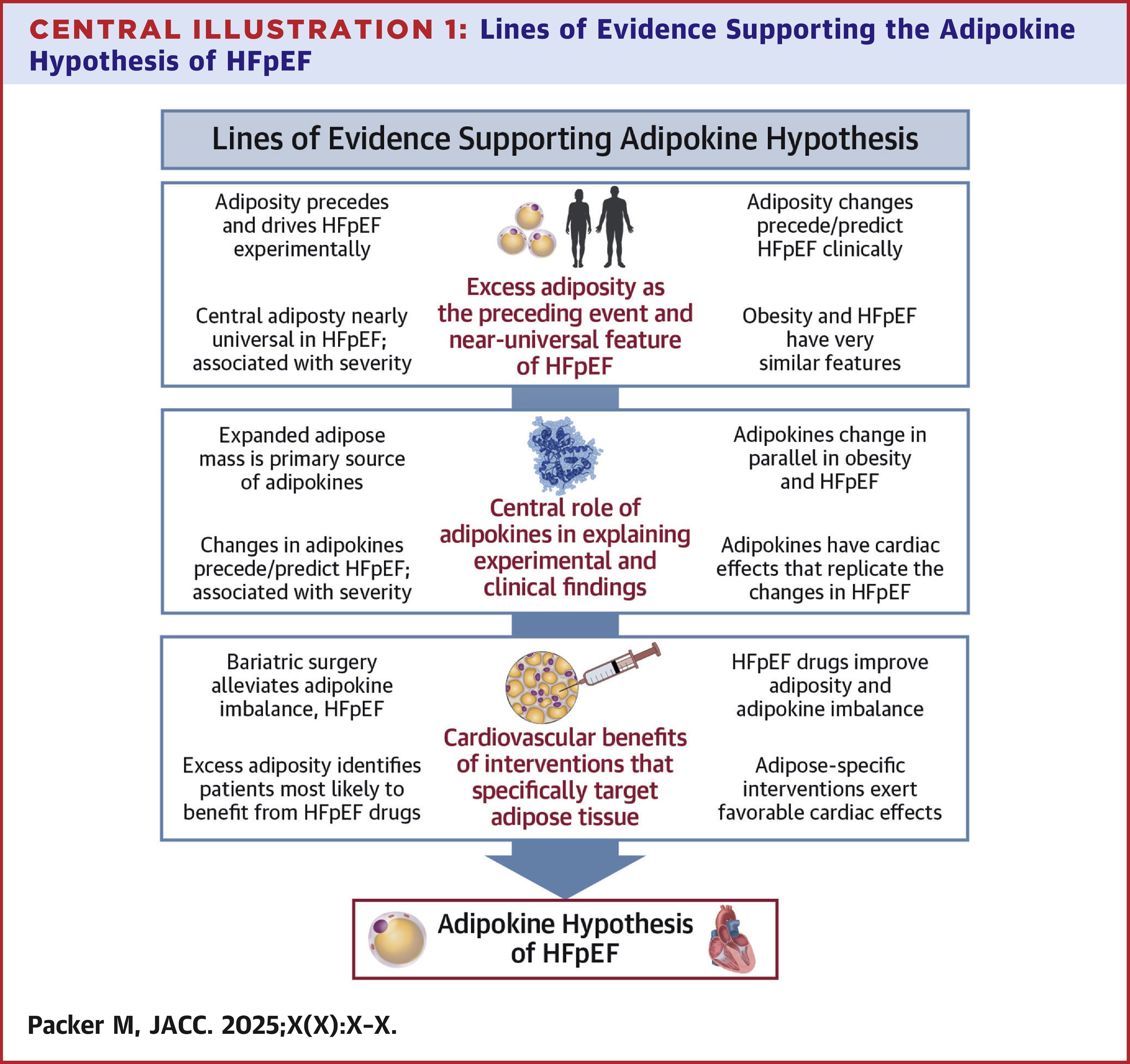
The adipokine hypothesis, first proposed in 2015, explains how fat cells (adipocytes) secrete signaling molecules that disrupt heart function. Excess visceral fat, in particular, increases levels of leptin and resistin while reducing adiponectin, a hormone that protects against inflammation. A 2021 study in Cardiology found that obese individuals had 2.3 times higher concentrations of pro-inflammatory adipokines compared to those with a healthy weight.

“Obesity isn’t just a risk factor—it’s a driver of the disease process,” said Dr. James Carter, a metabolic disease researcher at Harvard T.H. Chan School of Public Health. “Even modest weight loss can improve diastolic function, but the challenge lies in sustaining long-term behavioral change.”
What Are the Implications for Patients and Clinicians?
Healthcare providers are increasingly prioritizing weight management as a first-line intervention for HFpEF. The American College of Cardiology (ACC) now recommends a 5–10% reduction in body weight for patients with early-stage HFpEF, citing a 2023 clinical trial in ACC.org that showed a 30% decrease in hospital readmissions among participants who achieved this goal.
However, challenges remain. A 2022 survey by the Heart Failure Society of America revealed that only 40% of HFpEF patients receive structured weight-loss counseling, highlighting gaps in care. “We need to treat obesity as a chronic disease, not a lifestyle choice,” said Dr. Lisa Nguyen, a cardiologist at Johns Hopkins Medicine. “This requires integrating nutritionists, behavioral therapists, and pharmacists into heart failure management teams.”
What’s Next for Research and Treatment?
Researchers are exploring targeted therapies to address the adipokine pathway. A phase II trial of a leptin antagonist, published in Nature Medicine, showed a 15% improvement in cardiac stiffness markers among obese participants with HFpEF. While promising, the drug is still years from approval.
For now, lifestyle interventions remain the cornerstone of prevention. The Centers for Disease Control and Prevention (CDC) emphasizes that combining diet, exercise, and sleep hygiene can reduce HFpEF risk by up to 40%, according to a 2023 meta-analysis in JAMA Internal Medicine.