{kind=link}
Radiocephalic Arteriovenous Fistulas in Older Patients: Assessing Frailty and Surgical Outcomes
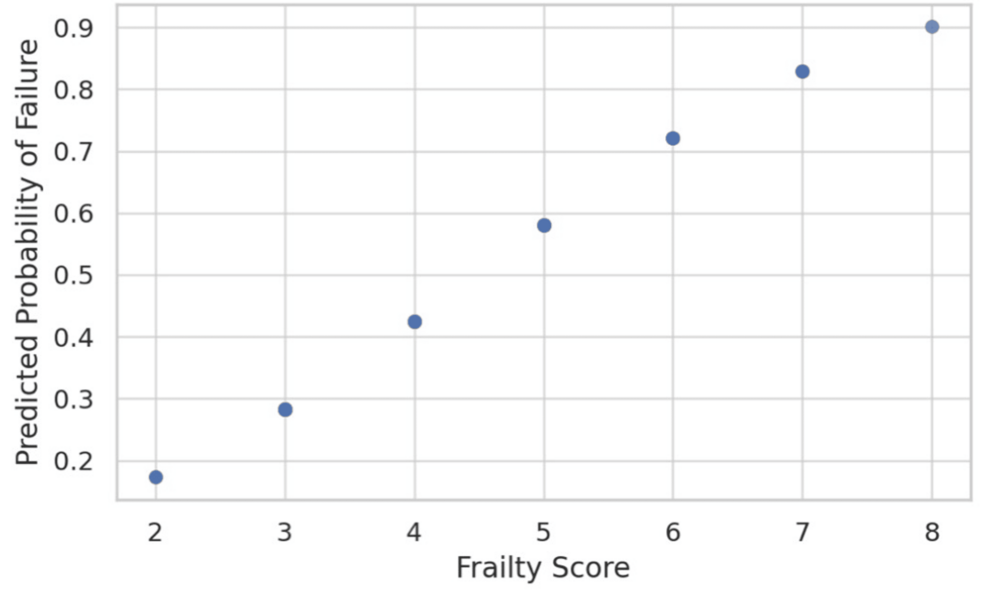
For patients aged 70 and older, the success of a radiocephalic arteriovenous fistula (RC-AVF)—the gold standard for hemodialysis access—is heavily influenced by the patient’s baseline frailty rather than age alone. Clinical research indicates that while age is a factor, frailty scores provide a more accurate prediction of whether a fistula will mature successfully or experience early failure. According to the National Kidney Foundation’s KDOQI guidelines, optimizing vascular access in the elderly requires a personalized approach that balances the durability of the access against the patient’s overall physiological reserve.
How Does Frailty Affect Fistula Maturation?
Frailty acts as a clinical marker for a patient’s limited ability to recover from the stress of surgery. In older adults, physiological decline often manifests as reduced vessel wall elasticity and slower healing responses. Data from the Journal of Vascular Access highlights that frail patients frequently experience higher rates of primary patency failure because the vein fails to dilate adequately to support the high blood flow required for dialysis. Surgeons are increasingly using tools like the Clinical Frailty Scale to assess whether a patient can withstand the maturation period, which can take several weeks, compared to the more immediate but higher-risk placement of central venous catheters.
Why Is the Radiocephalic Fistula Preferred?
The radiocephalic fistula, which connects the radial artery to the cephalic vein at the wrist, remains the preferred initial access for hemodialysis across all age groups. According to the American Society of Nephrology, the RC-AVF is associated with the lowest rates of infection and thrombosis compared to other access types, such as prosthetic grafts or tunneled catheters. For patients over 70, the challenge lies in the quality of the vasculature. Atherosclerosis and long-term hypertension often render distal veins unsuitable, leading surgeons to sometimes opt for more proximal access, such as brachiocephalic fistulas, to ensure a higher chance of success despite the increased risk of steal syndrome.
Comparison of Access Outcomes in Older Adults
Clinical decision-making often involves weighing the benefits of different access types based on patient health status. The table below summarizes the trade-offs typically observed in clinical practice.
| Access Type | Pros | Cons |
|---|---|---|
| Radiocephalic AVF | Lowest infection risk, best long-term survival | High primary failure rate in frail, elderly vessels |
| Brachiocephalic AVF | Higher blood flow, easier to mature | Increased risk of heart failure and steal syndrome |
| Central Venous Catheter | Immediate use | High infection risk, high mortality, vascular stenosis |
Clinical Considerations for Long-Term Patency
Maintaining a functioning fistula in the elderly requires diligent post-operative monitoring. The Vascular Society emphasizes that early ultrasound surveillance is critical to identify narrowing or “stenosis” before the fistula fails completely. For patients aged 70 and above, the decision to intervene must be weighed against the patient’s life expectancy and overall quality of life. If a fistula shows signs of poor maturation, clinicians often perform balloon angioplasty to salvage the access. However, in highly frail patients, repetitive interventions can become burdensome, leading care teams to discuss the possibility of “dialysis-minimal” or conservative management strategies in specific, advanced cases.
Key Takeaways for Patients and Providers
- Frailty over Chronology: A patient’s biological frailty score is often more predictive of surgical success than their chronological age.
- Early Surveillance: Post-operative ultrasound is essential to catch early maturation issues before they result in total fistula thrombosis.
- Individualized Planning: Vascular access should be planned months before the expected start of dialysis to allow for maturation or potential revision.
- Risk Mitigation: While RC-AVFs have the best safety profile, surgeons must frequently assess venous anatomy to determine if a more proximal fistula is necessary to ensure reliable dialysis.