{kind=link}
Understanding Plasmodium vivax Malaria Relapse and Thrombocytopenia
Plasmodium vivax malaria can cause clinical relapse months or years after an initial infection, even in patients living in non-endemic regions. Clinicians must maintain a high index of suspicion for this parasite when patients present with thrombocytopenia—a low platelet count—and a history of travel to areas where the disease is common. According to the Centers for Disease Control and Prevention (CDC), P. vivax is unique because it forms dormant liver stages, known as hypnozoites, that can reactivate long after the primary infection has cleared.
How Does Plasmodium vivax Cause Relapse?
The primary mechanism behind P. vivax relapse is the activation of hypnozoites. Unlike Plasmodium falciparum, which does not have a dormant liver stage, P. vivax parasites can remain inactive in the liver for weeks to years. When these hypnozoites “wake up,” they release merozoites into the bloodstream, triggering a new symptomatic infection. Research published in the World Health Organization (WHO) Malaria Report highlights that this biological trait makes P. vivax particularly difficult to eliminate, as standard blood-stage treatments do not target the dormant liver reservoir.

Why Is Thrombocytopenia a Clinical Red Flag?
Thrombocytopenia, or a significant drop in blood platelet counts, is a hallmark clinical finding in many malaria cases, including those caused by P. vivax. Data from the National Library of Medicine suggest that platelet destruction in malaria occurs through several mechanisms, including immune-mediated clearance and sequestration in the spleen. While thrombocytopenia is often associated with severe malaria, it frequently appears in non-severe cases as well, serving as an important diagnostic clue for clinicians who might otherwise overlook malaria in patients who have returned from endemic regions.
Clinical Management in Non-Endemic Areas
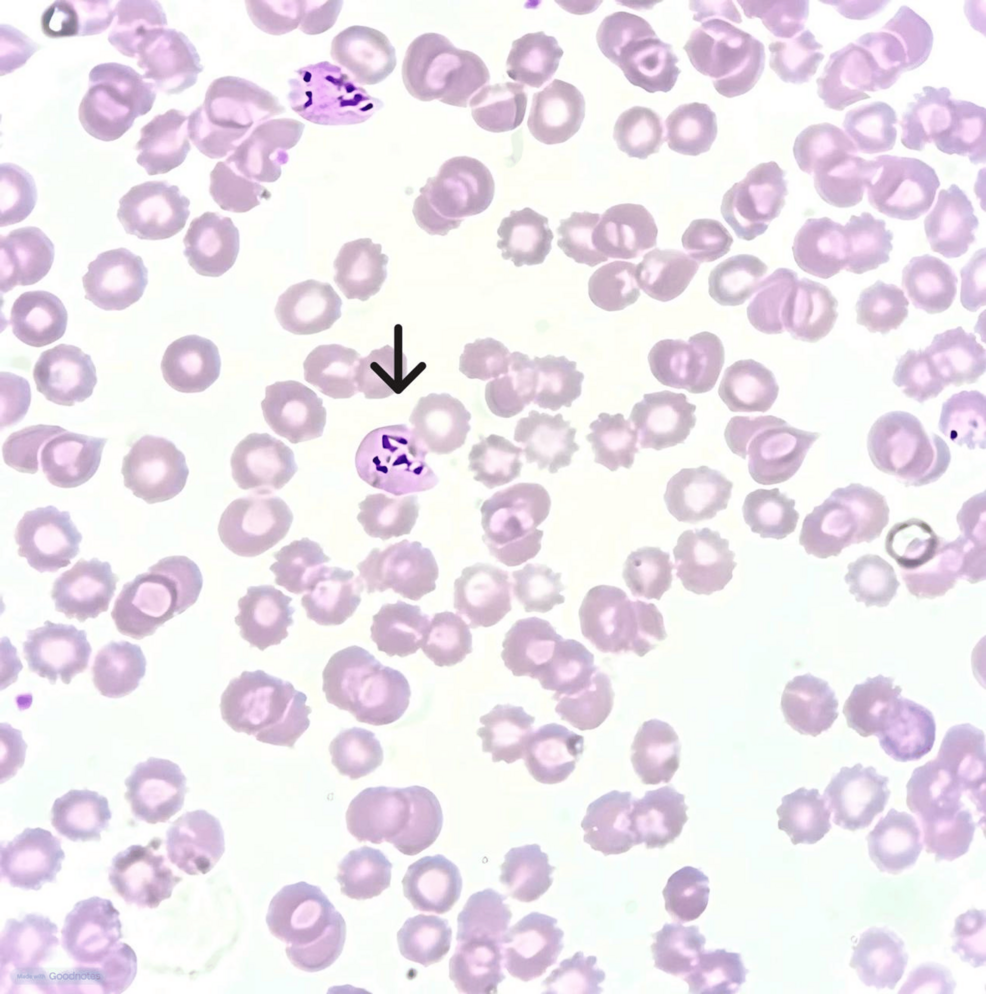
In regions where malaria is not endemic, such as the United States or parts of Europe, physicians may not immediately consider a parasitic infection. Diagnosing a relapse requires a detailed travel history and specific laboratory testing. The CDC recommends using thin and thick blood smears for microscopic identification of the parasite. In cases where microscopy is inconclusive, molecular testing via polymerase chain reaction (PCR) can confirm the presence of P. vivax DNA.
Key Diagnostic Considerations
- Travel History: Always ask patients about travel to malaria-endemic regions, even if that travel occurred years ago.
- Hypnozoite Clearance: Treatment for P. vivax must include drugs that target the liver stage, such as primaquine or tafenoquine, alongside blood-stage medications.
- Glucose-6-Phosphate Dehydrogenase (G6PD) Deficiency: Before administering primaquine or tafenoquine, patients must be tested for G6PD deficiency to avoid the risk of severe hemolytic anemia.
Comparing Malaria Species and Relapse Risk
| Feature | Plasmodium vivax | Plasmodium falciparum |
|---|---|---|
| Dormant Liver Stage | Yes (Hypnozoites) | No |
| Risk of Relapse | High | None |
| Common Symptoms | Fever, chills, thrombocytopenia | Fever, severe anemia, organ failure |
The clinical presentation of P. vivax relapse—often characterized by thrombocytopenia and cyclical fever—demands prompt identification to prevent complications. Because the parasite can remain dormant for extended periods, clinicians should not rule out malaria solely based on a distant travel history. Early diagnosis and the administration of appropriate radical cure therapy remain the standards of care for preventing future relapses.