{kind=link}
Point-of-care ultrasound (POCUS) has become a valuable diagnostic tool in emergency medicine for identifying anorectal infections, such as perianal abscesses. By providing real-time imaging, clinicians can differentiate between simple abscesses and more complex pathologies, potentially reducing the need for expensive or time-consuming diagnostic imaging like computed tomography (CT) scans.
Diagnostic Utility of POCUS in Emergency Settings
Emergency department clinicians frequently encounter patients presenting with perianal pain, swelling, and fever. According to research published in the Journal of Emergency Medicine, physical examination alone can sometimes be limited, particularly when an abscess is deep or obscured by significant inflammation. POCUS allows physicians to visualize fluid collections, assess the size of an abscess, and determine its proximity to the anal sphincter.
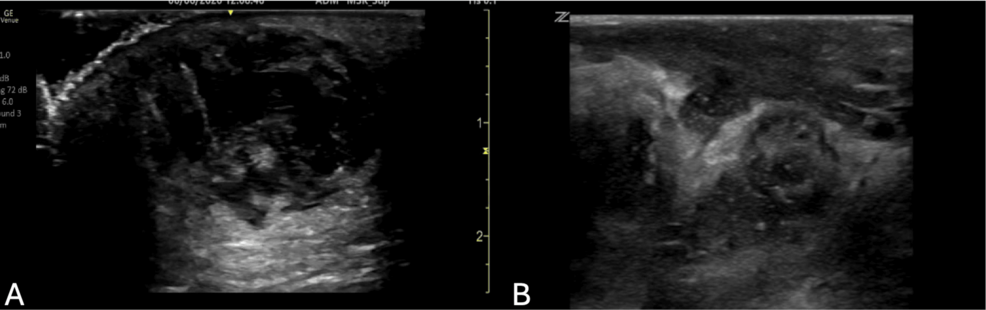
The use of ultrasound in this context is supported by the American College of Emergency Physicians (ACEP), which recognizes POCUS as an extension of the physical exam. When performed by a trained provider, ultrasound can identify the presence of a hypoechoic (dark) fluid collection, which is a hallmark of an abscess. This immediate visual confirmation helps clinicians decide whether an incision and drainage procedure can be performed at the bedside or if a surgical consultation is required.
Comparing POCUS to Traditional Imaging
Historically, when a physical exam was inconclusive, emergency physicians often ordered a CT scan to confirm the diagnosis of an anorectal abscess. However, as noted by the American Journal of Roentgenology, CT scans involve ionizing radiation and increased costs.
POCUS offers several distinct advantages:
- No Radiation Exposure: Unlike CT, ultrasound uses sound waves to create images, eliminating radiation risks for the patient.
- Rapid Results: POCUS provides immediate answers, which is critical in an emergency setting where patient turnover and timely intervention are priorities.
- Dynamic Assessment: Clinicians can use the ultrasound probe to apply gentle pressure, helping them distinguish between a fluid-filled abscess and solid tissue or bowel loops.
Limitations and Clinical Considerations
While POCUS is a powerful tool, it is operator-dependent. The accuracy of the diagnosis relies on the clinician’s training and experience with ultrasound technology. Furthermore, some deep or complex infections may still require advanced imaging like MRI or CT to fully map the extent of the disease, especially if there is suspicion of a fistula or systemic involvement.
According to guidelines from the Infectious Diseases Society of America (IDSA), the management of anorectal infections should always prioritize drainage of the abscess and appropriate antibiotic therapy when indicated by clinical signs of systemic infection or immunocompromise. POCUS serves as an adjunct to these clinical practices, not as a replacement for surgical judgment or comprehensive patient evaluation.
Key Takeaways for Clinical Practice
- Immediate Identification: POCUS is effective for the rapid identification of perianal abscesses in the emergency department.
- Reduced Resource Utilization: Increased use of POCUS may decrease reliance on CT imaging, thereby reducing radiation exposure and lowering healthcare costs.
- Training Requirement: Consistent training and competency assessment are necessary for emergency medicine practitioners to ensure diagnostic accuracy.
- Clinical Integration: Ultrasound findings must be interpreted alongside the patient’s history and physical examination results to guide appropriate management decisions.
Related reading