{kind=link}
Pulmonary Mucormycosis: Understanding a Rare but Serious Fungal Infection in Diabetic Patients
Pulmonary mucormycosis is a rare, aggressive, and life-threatening fungal infection that primarily affects individuals with compromised immune systems. While relatively uncommon, its incidence has historically been higher among patients with poorly controlled diabetes mellitus. Understanding the clinical presentation, risk factors, and the necessity of prompt intervention is critical for both patients and healthcare providers.
What is Pulmonary Mucormycosis?
Mucormycosis is a serious infection caused by a group of molds known as mucormycetes. These fungi are ubiquitous in the environment, commonly found in soil, decaying organic matter, and even air. While most people are exposed to these spores daily without consequence, individuals with underlying health conditions—particularly uncontrolled diabetes—are at a significantly higher risk of the spores invading the lung tissue and causing pulmonary mucormycosis.
The infection begins when the spores are inhaled into the lungs. In a healthy immune system, the body’s defenses easily neutralize these invaders. However, in patients with metabolic imbalances or suppressed immunity, the fungus can proliferate, leading to tissue necrosis, blood vessel invasion (angioinvasion), and potentially systemic dissemination.
The Link Between Diabetes and Fungal Infections
There is a well-documented connection between uncontrolled diabetes mellitus and an increased susceptibility to mucormycosis. Specifically, patients with diabetic ketoacidosis (DKA) are at the highest risk. The acidic environment and high levels of glucose in the blood impair the function of neutrophils—the white blood cells responsible for fighting off fungal infections. High glucose levels provide a nutrient-rich environment that promotes the rapid growth of the mold.
Clinical Presentation and Diagnostic Challenges
One of the primary challenges in managing pulmonary mucormycosis is that its symptoms often mimic common respiratory issues, such as bacterial pneumonia. Patients frequently present with:
- Persistent cough, sometimes producing blood-stained sputum (hemoptysis)
- Fever that does not respond to standard antibiotics
- Chest pain or shortness of breath
- Fatigue and general malaise
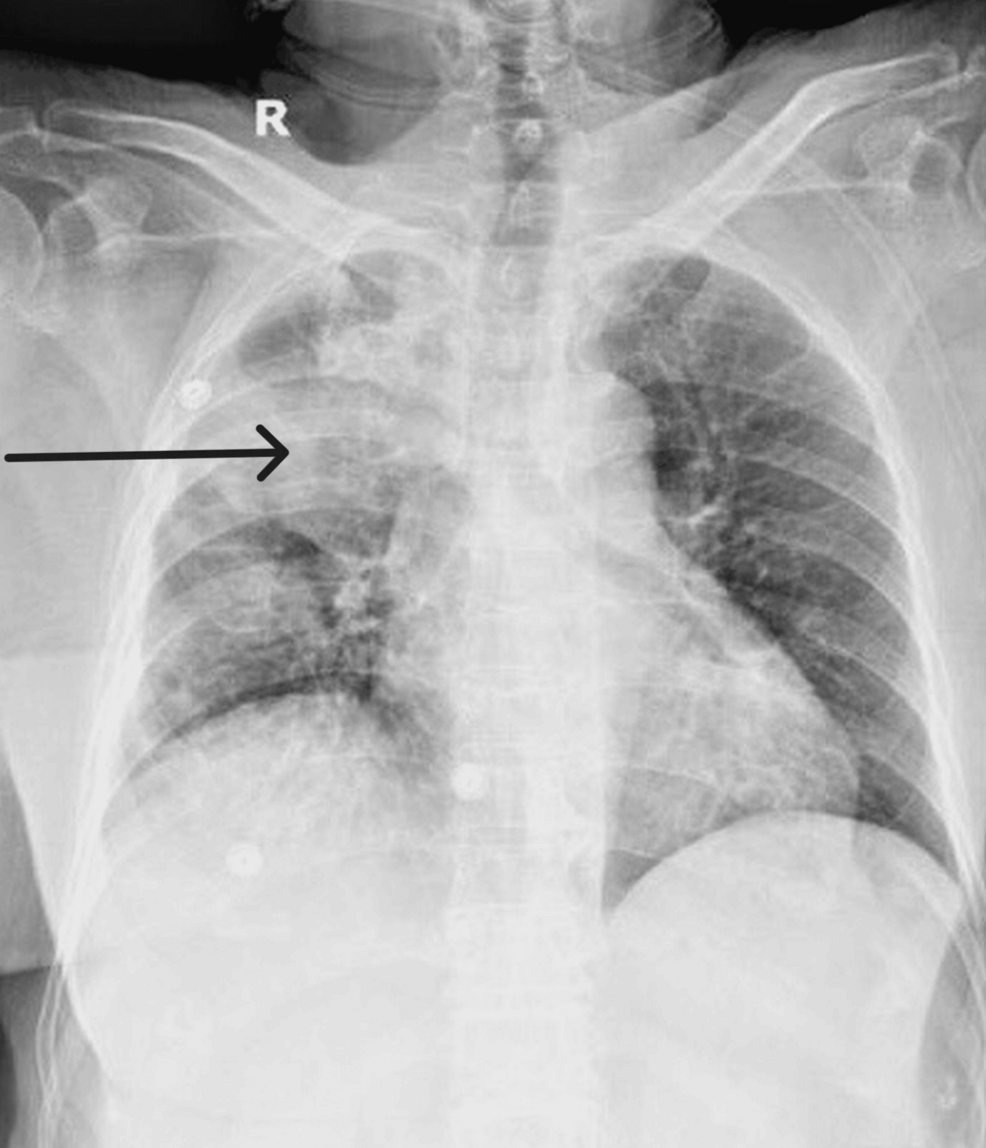
Because these symptoms are non-specific, patients are often initially treated for community-acquired pneumonia. When the “pneumonia” fails to resolve after multiple courses of antibiotics, clinicians must maintain a high index of suspicion for fungal pathogens. Diagnostic imaging, such as a CT scan of the chest, may reveal characteristic findings like the “halo sign,” which suggests localized tissue invasion.
Key Takeaways for Patients and Providers
- Early Detection is Vital: If a patient with diabetes develops pneumonia symptoms that do not improve within 48–72 hours of antibiotic treatment, further investigation is required.
- Glycemic Control: Maintaining stable blood glucose levels is the most effective preventative measure against invasive fungal infections.
- Multidisciplinary Care: Management typically requires a combination of surgical debridement of infected tissue, aggressive antifungal therapy (usually with amphotericin B), and strict management of the underlying diabetes.
- High Mortality Risk: Due to its rapid progression and ability to invade blood vessels, pulmonary mucormycosis carries a high mortality rate, making early surgical and medical intervention non-negotiable.
Frequently Asked Questions (FAQ)
Can mucormycosis be spread from person to person?
No, mucormycosis is not contagious. It is acquired through the inhalation or ingestion of fungal spores from the environment, not through contact with infected individuals.


Why is it so hard to diagnose?
It is tricky to diagnose because the symptoms are identical to other, more common lung infections. Standard blood tests often fail to detect the fungus, requiring tissue biopsies or specialized imaging for an accurate diagnosis.
What is the role of surgery in treatment?
Because the fungus causes localized tissue death (necrosis), antifungal medications alone may not reach the site of infection effectively. Surgical removal of the infected lung tissue is often necessary to stop the spread of the fungus.
Moving Forward
Pulmonary mucormycosis remains a formidable challenge in clinical medicine. As clinicians, our focus must remain on the early identification of high-risk patients and the rapid escalation of care when standard treatments for pneumonia fail. For patients living with diabetes, the most powerful tool remains consistent blood sugar management, which significantly reduces the risk of allowing opportunistic infections to take hold. If you or a loved one are experiencing persistent respiratory symptoms, consult a healthcare professional immediately to rule out serious complications.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
Related reading