{kind=link}
Severe secondary hyperparathyroidism in patients on chronic hemodialysis can lead to spontaneous quadriceps tendon rupture due to systemic mineral and bone disorder (CKD-MBD). This rare complication occurs when uncontrolled parathyroid hormone (PTH) levels degrade tendon collagen and weaken musculoskeletal integrity, often necessitating surgical repair and aggressive medical management of calcium and phosphate levels.
The Link Between Kidney Failure and Tendon Rupture
Patients with end-stage renal disease (ESRD) frequently develop secondary hyperparathyroidism. According to the National Center for Biotechnology Information (NCBI), this happens when the kidneys can’t activate vitamin D or eliminate phosphorus, triggering the parathyroid glands to overproduce parathyroid hormone (PTH) to maintain calcium balance.

While PTH focuses on bone turnover, extreme levels affect soft tissues. High PTH concentrations increase the activity of osteoclasts and can lead to the deposition of calcium-phosphate crystals in tendons. This process, known as ectopic calcification, makes tendons brittle. When a tendon loses its elasticity, it can snap during routine movement—a “spontaneous” rupture—without a significant traumatic event.
Identifying Quadriceps Tendon Rupture in Dialysis Patients
A quadriceps tendon rupture separates the quadriceps muscle from the patella (kneecap). In patients with chronic kidney disease (CKD), the presentation often includes a sudden “pop” sensation followed by an inability to extend the knee. According to clinical reports in Cureus, physical examination typically reveals a palpable gap above the patella and a visible “sag” in the thigh muscle.

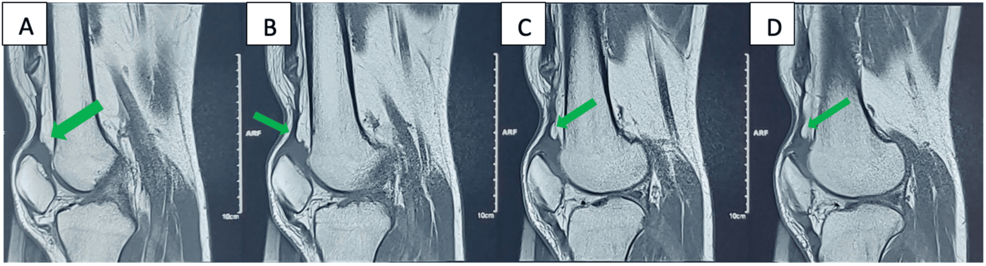
Diagnosis is confirmed through imaging. Ultrasound and Magnetic Resonance Imaging (MRI) are the gold standards for visualizing the extent of the tear and the degree of calcification within the tendon. These tools allow surgeons to determine if the tendon is completely severed or partially torn.
Managing Secondary Hyperparathyroidism and CKD-MBD
Treating the rupture is only half the battle; the underlying metabolic instability must be addressed to prevent further ruptures. The Kidney Disease: Improving Global Outcomes (KDIGO) guidelines emphasize the management of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD).
Medical teams typically employ three primary strategies to stabilize the patient:
- Phosphate Binders: Medications taken with meals to prevent the absorption of phosphorus from food.
- Vitamin D Analogs: Calcitriol or other active vitamin D supplements to suppress the overproduction of PTH.
- Calcimimetics: Drugs like cinacalcet that trick the parathyroid gland into thinking there is enough calcium in the blood, thereby lowering PTH levels.
In severe cases where medication fails, a parathyroidectomy—the surgical removal of one or more parathyroid glands—may be required to prevent systemic complications.
Surgical Recovery and Long-Term Outlook
Surgical repair of the quadriceps tendon involves reattaching the tendon to the patella using heavy sutures. However, recovery in hemodialysis patients is often slower than in the general population. Poor protein synthesis and impaired wound healing, common in ESRD, increase the risk of post-operative infections and graft failure.
Post-operative rehabilitation focuses on gradual range-of-motion exercises. Physical therapists must balance the need for mobility with the fragility of the repaired tissue, especially if the patient’s PTH levels remain elevated during the healing phase.
Comparison of Metabolic Markers in Tendon Health
| Marker | Normal Range/Function | Impact in Severe Hyperparathyroidism |
|---|---|---|
| PTH Level | Regulates Calcium/Phosphorus | Excessive levels trigger bone resorption and tendon degradation. |
| Serum Phosphorus | Essential Mineral | Hyperphosphatemia leads to ectopic calcification of soft tissues. |
| Calcium | Structural Support | Imbalance leads to “hungry bone syndrome” or vascular calcification. |
Frequently Asked Questions
Can a ruptured tendon heal without surgery in dialysis patients?
While small partial tears may be managed conservatively, a complete spontaneous rupture usually requires surgical intervention to restore the ability to walk and stand.

Why does dialysis cause these issues?
Dialysis cleans the blood but does not replace the endocrine functions of the kidney, such as producing active vitamin D, which is critical for bone and tendon health.
What are the warning signs of tendon weakness?
Patients should report persistent stiffness, localized pain in the knee, or a decrease in leg strength to their nephrologist immediately.
Related reading