{kind=link}
Cerebral Venous Sinus Thrombosis: A Rare Complication of Pneumococcal Meningitis
Cerebral venous sinus thrombosis (CVST) is a rare but life-threatening neurological complication occurring in patients diagnosed with bacterial meningitis, particularly when caused by Streptococcus pneumoniae. While bacterial meningitis primarily involves inflammation of the protective membranes covering the brain and spinal cord, the infection can trigger a hypercoagulable state—an increased tendency for blood to clot—leading to the formation of thrombi within the brain’s venous drainage system. Early identification through neuroimaging is essential for survival and the prevention of permanent neurological deficits.
What is the link between pneumococcal meningitis and CVST?
The association between Streptococcus pneumoniae and CVST stems from the severe inflammatory response triggered by the infection. According to the National Institutes of Health (NIH), bacterial meningitis induces a systemic inflammatory cascade that alters the body’s coagulation pathways. When the infection spreads to the intracranial venous sinuses, the combination of endothelial damage (injury to the lining of the blood vessels) and blood stasis facilitates clot formation. This prevents the brain from draining blood effectively, leading to increased intracranial pressure, swelling, and potential venous infarction.

How is the condition diagnosed?
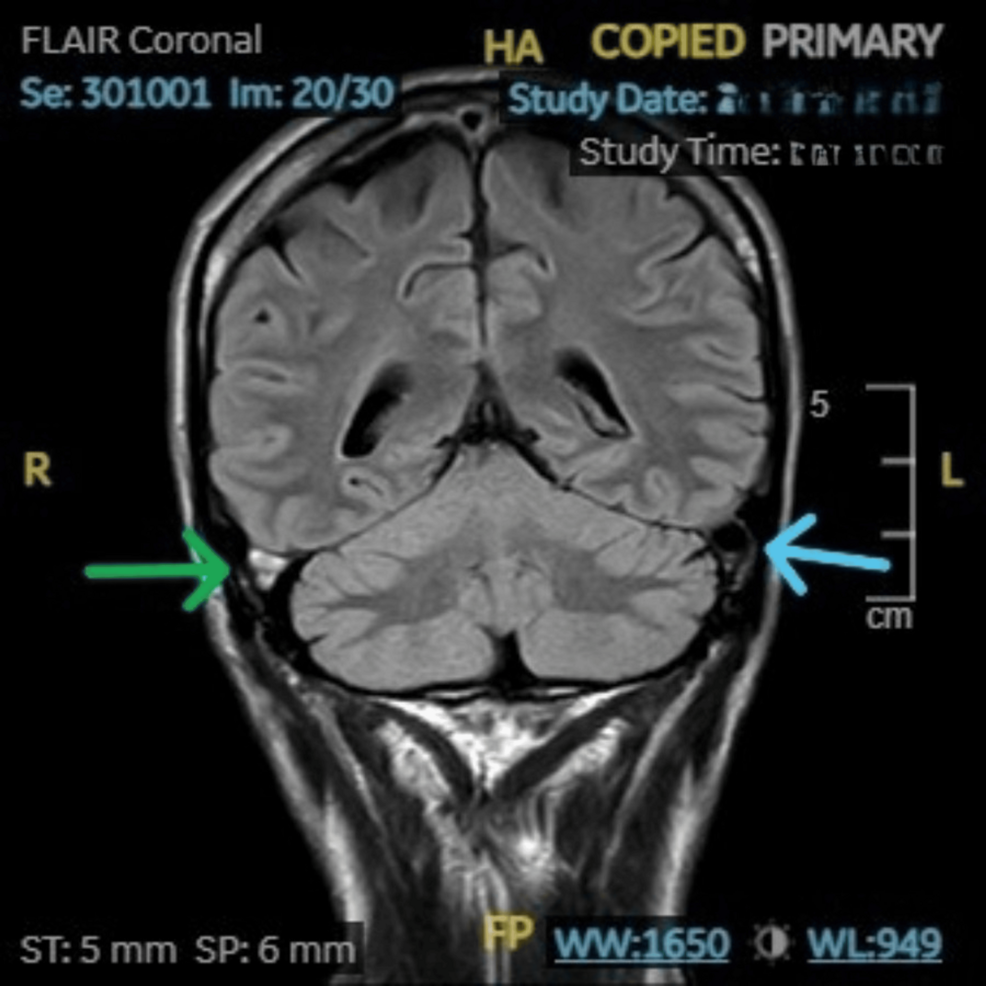
Clinical symptoms of CVST in meningitis patients are often masked by the underlying infection, which may include fever, neck stiffness, and altered mental status. Medical experts rely on advanced imaging to confirm the diagnosis. The American Heart Association notes that Magnetic Resonance Venography (MRV) or Computed Tomography Venography (CTV) are the gold standards for visualizing the venous sinuses. These scans allow clinicians to detect blockages that standard imaging might miss, providing the definitive evidence needed to initiate life-saving interventions.

What are the standard treatment approaches?
Treatment for CVST secondary to meningitis requires a delicate balance between managing the infection and addressing the blood clot. The primary approach involves:

- Antibiotic Therapy: Aggressive intravenous antibiotics are required to eradicate the Streptococcus pneumoniae infection, which acts as the underlying driver of the inflammatory process.
- Anticoagulation: According to clinical guidelines published in The Lancet Neurology, anticoagulation therapy is generally indicated for patients with CVST, even in the presence of small intracranial hemorrhages, to prevent further clot propagation and venous occlusion.
- Supportive Care: Managing intracranial pressure through elevation of the head, fluid management, and, in severe cases, surgical decompression, may be necessary to minimize brain injury.
Key Takeaways
- High Risk: Pneumococcal meningitis is a significant, albeit rare, risk factor for developing secondary cerebral venous sinus thrombosis.
- Clinical Vigilance: Patients who fail to show expected neurological improvement despite appropriate antibiotic treatment for meningitis should be evaluated for potential CVST.
- Imaging is Critical: MRV or CTV are necessary to accurately diagnose venous sinus involvement and distinguish it from other meningitis complications like brain abscesses or strokes.
- Multidisciplinary Care: Management requires collaboration between infectious disease specialists, neurologists, and neurosurgeons to address both the infection and the vascular obstruction.
The prognosis for patients with CVST following pneumococcal meningitis depends heavily on the speed of diagnosis and the initiation of targeted therapy. While the condition remains uncommon, clinicians maintain a high index of suspicion for patients presenting with persistent focal neurological deficits or unexplained clinical decline. Ongoing research continues to refine the use of anticoagulants in the context of central nervous system infections to improve long-term patient outcomes.
Worth a look