{kind=link}
Acute Pancreatitis as an Atypical Presentation of Plasma Cell Leukemia
Plasma cell leukemia (PCL) is a rare and aggressive form of multiple myeloma characterized by the presence of circulating malignant plasma cells in the peripheral blood. While typically presenting with symptoms like bone pain, fatigue, and renal insufficiency, recent clinical reports highlight rare instances where patients present with acute pancreatitis. Recognizing these atypical manifestations is critical for early diagnosis and intervention in young, otherwise healthy patients.
What is Plasma Cell Leukemia?
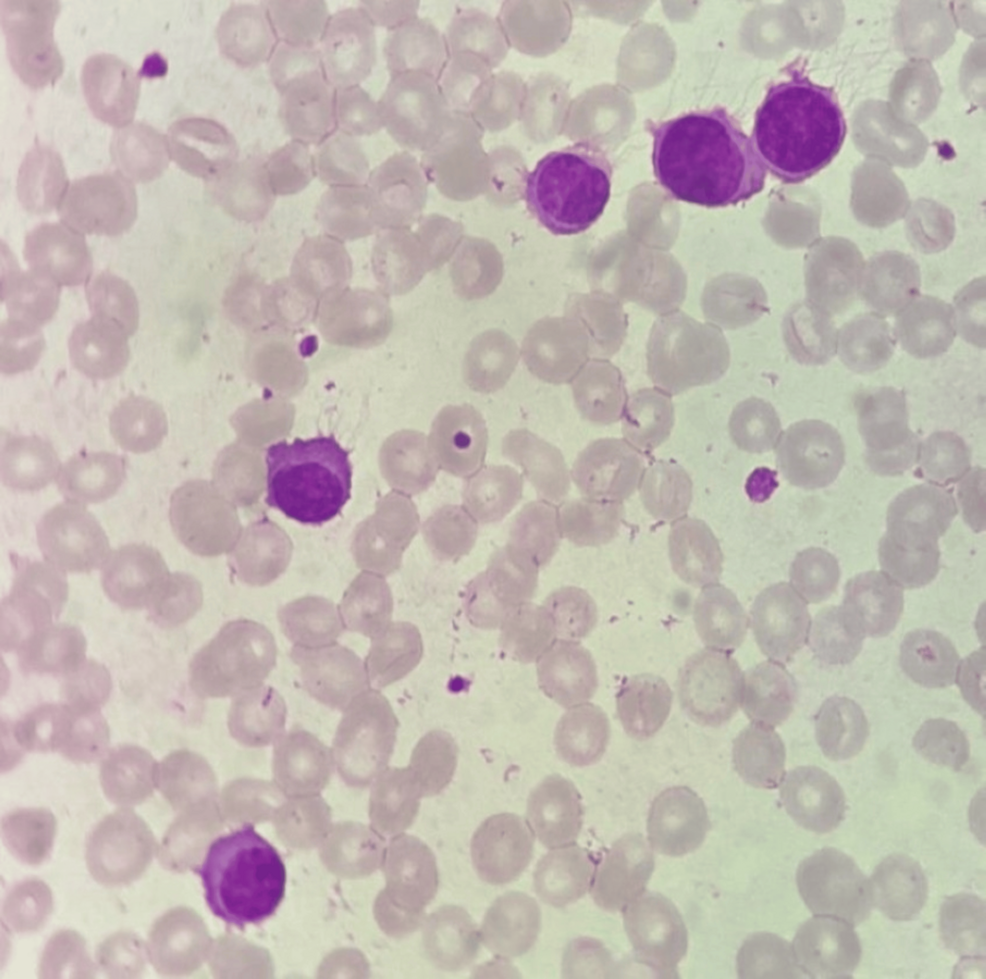
Plasma cell leukemia occurs when abnormal plasma cells—a type of white blood cell responsible for producing antibodies—proliferate uncontrollably and spill into the bloodstream. According to the American Cancer Society, PCL is defined by a circulating plasma cell count of at least 2,000 cells per microliter or more than 20% of the peripheral white blood cell differential. It is classified into two types: primary PCL, which arises de novo, and secondary PCL, which represents an aggressive transformation of pre-existing multiple myeloma.

The condition is notoriously difficult to treat. Because it is a systemic malignancy, it often involves multiple organ systems, leading to complications that may mask the underlying blood disorder during the initial clinical assessment.
How Can PCL Cause Acute Pancreatitis?
Acute pancreatitis is an inflammation of the pancreas that typically results from gallstones or heavy alcohol use. However, in the context of plasma cell leukemia, pancreatitis can occur due to hypercalcemia or direct infiltration of malignant cells into the pancreatic tissue.

When malignant plasma cells infiltrate the pancreas, they can obstruct the pancreatic ducts, leading to the premature activation of digestive enzymes. This process causes autodigestion of the organ, resulting in severe abdominal pain and elevated lipase levels. Furthermore, clinical studies published in the Journal of Hematology and Oncology note that the high tumor burden associated with PCL can lead to metabolic derangements, such as severe hypercalcemia, which is a known independent risk factor for the development of acute pancreatitis.
Diagnostic Challenges in Young Patients
Diagnosing PCL in young patients often proves difficult because the disease is significantly more common in older adults, typically those over age 60. Clinicians may not prioritize hematologic malignancy in a young patient presenting with acute abdominal symptoms.
- Atypical Symptoms: Patients may present with abdominal pain, nausea, or vomiting, which leads physicians to investigate common gastrointestinal causes first.
- Imaging Limitations: Standard CT scans may show pancreatic swelling, which does not immediately distinguish between inflammatory pancreatitis and malignant infiltration.
- Blood Work: A simple complete blood count (CBC) may show anemia or leukocytosis, but specific markers like serum protein electrophoresis (SPEP) or bone marrow biopsy are required to confirm the presence of monoclonal plasma cells.
Clinical Management and Prognosis
The management of PCL requires immediate, intensive intervention. According to guidelines from the International Myeloma Foundation, treatment typically involves multi-agent induction chemotherapy, often followed by an autologous stem cell transplant for eligible patients.

Because PCL is highly aggressive, the prognosis remains guarded. Early detection of systemic symptoms—even those that appear gastrointestinal in origin—can allow for the initiation of targeted therapies, such as proteasome inhibitors and immunomodulatory drugs, which may improve survival outcomes.
Summary of Key Clinical Considerations
| Feature | Clinical Significance |
|---|---|
| Primary Presentation | Often systemic (bone pain, fatigue), but can be localized (pancreatitis). |
| Diagnostic Marker | Circulating plasma cells >2,000/µL or >20% of WBC count. |
| Treatment Focus | Rapid cytoreduction via intensive chemotherapy and stem cell support. |
For clinicians, the appearance of acute pancreatitis in a patient without typical risk factors should prompt a broader investigation. Incorporating a peripheral blood smear and serum protein studies into the workup of unexplained abdominal inflammation may be the deciding factor in identifying a hematologic emergency.
Worth a look