{kind=link}
Sudden Infant Death Syndrome (SIDS) often involves a complex interaction between an infant’s biological vulnerability and external stressors, including inflammation from respiratory infections. According to the National Institutes of Health (NIH), this inflammatory response can impair a baby’s ability to wake up or breathe during sleep, contributing to fatal events in vulnerable infants.
Medical researchers have shifted from viewing SIDS as a single cause to seeing it as a convergence of factors. While environmental triggers like stomach-sleeping are well-known, the underlying biological state of the infant—specifically how their immune system handles inflammation—plays a critical role in whether a stressor becomes fatal.
How does inflammation contribute to SIDS?
Inflammation acts as both a trigger and a marker of vulnerability in SIDS cases. When an infant fights a viral or bacterial infection, the body releases proteins called cytokines. According to research published in PubMed, an overactive or dysfunctional inflammatory response can affect the brainstem, specifically the areas that control arousal and breathing.
If a baby’s brain doesn’t signal them to wake up when oxygen levels drop (hypoxia), they can’t clear their airway or shift positions. Inflammation can blunt this “wake-up call.” It doesn’t cause SIDS on its own, but it creates a physiological state where a baby is less likely to survive a breathing obstruction.
What is the Triple Risk Model of SIDS?
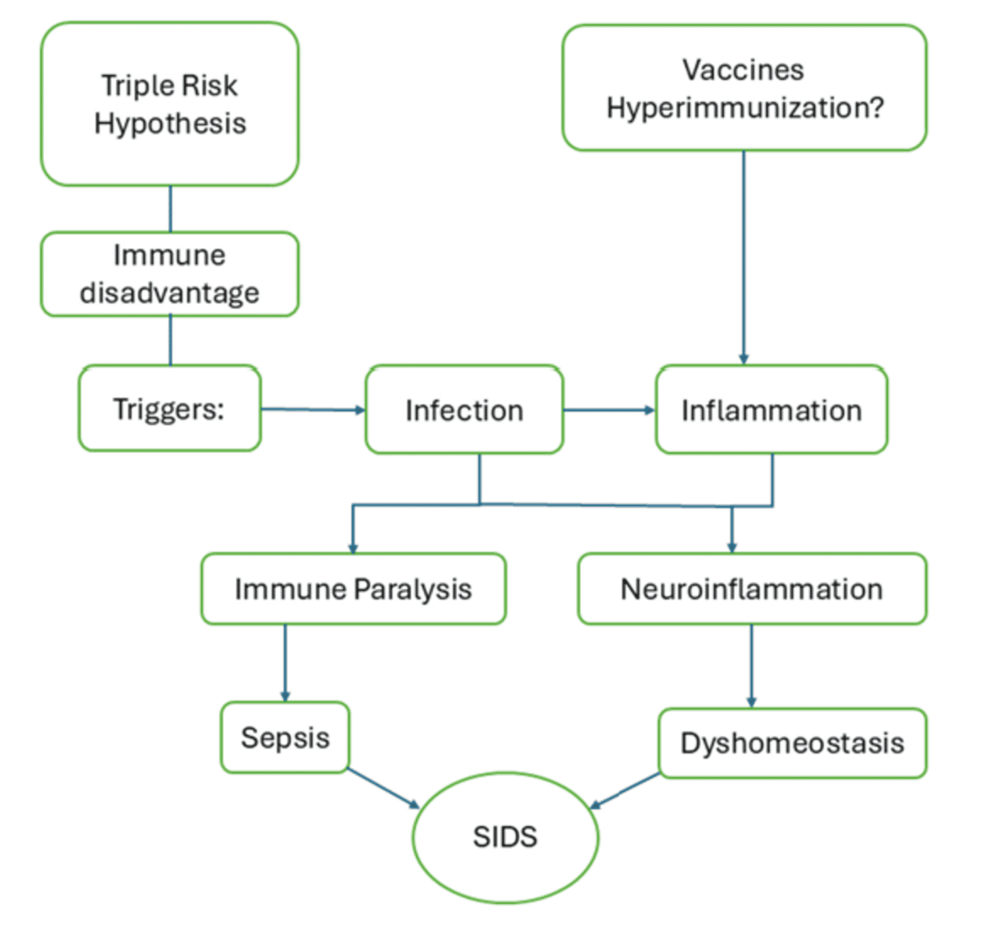
The Triple Risk Model, a framework widely accepted in pediatric research, suggests that SIDS occurs only when three specific factors overlap. According to the National Center for Biotechnology Information (NCBI), these factors are:
- A Vulnerable Infant: The baby has an underlying biological abnormality, often involving the serotonin system or an impaired immune response.
- A Critical Developmental Period: The first six months of life, when the infant’s respiratory and neurological systems are maturing rapidly.
- An Exogenous Stressor: An external trigger, such as a respiratory infection, overheating, or prone sleep positioning.
Inflammation fits into this model as both a vulnerability and a stressor. A baby with a genetic predisposition to poor inflammatory control is more vulnerable. Simultaneously, a common cold (an inflammatory event) can be the final stressor that triggers a fatal event.
Which biomarkers are linked to infant respiratory distress?
Researchers look for specific biomarkers in lung tissue and blood to understand the inflammatory process in SIDS. Pro-inflammatory cytokines, such as Interleukin-6 (IL-6) and Tumor Necrosis Factor-alpha (TNF-α), are frequently elevated in SIDS autopsies. These markers indicate that the infant’s immune system was fighting an infection shortly before death.
The contrast in findings is telling. In healthy infants, inflammation is a controlled process that resolves. In SIDS cases, the inflammatory response often appears dysregulated. This suggests that the problem isn’t the infection itself, but how the infant’s body reacts to it.
Comparing Biological and Environmental Risk Factors
| Factor Type | Examples | Role in SIDS |
|---|---|---|
| Biological (Internal) | Cytokine imbalance, Serotonin deficiency | Creates the “Vulnerable Infant” state. |
| Environmental (External) | Soft bedding, Prone sleeping, Smoking | Acts as the “Exogenous Stressor.” |
| Inflammatory (Combined) | Upper respiratory infection, Fever | Increases vulnerability and acts as a trigger. |
How can parents reduce SIDS risk?
While parents can’t control a baby’s genetic inflammatory response, they can eliminate the external stressors that interact with that biology. The American Academy of Pediatrics (AAP) provides clear, evidence-based guidelines to lower the risk of SIDS.

- Back to Sleep: Always place babies on their backs for every sleep.
- Clear the Crib: Keep the sleep area free of blankets, pillows, bumper pads, and stuffed toys.
- Firm Surface: Use a firm, flat sleep surface (like a safety-approved crib mattress) covered only by a fitted sheet.
- Room Sharing: Share a room—but not a bed—with the infant for at least the first six months.
- Avoid Overheating: Keep the room at a comfortable temperature and avoid over-bundling the baby.
Frequently Asked Questions
Can a common cold increase the risk of SIDS?
Yes. While most colds are harmless, the inflammation associated with respiratory infections can act as an exogenous stressor. For a vulnerable infant, this can impair the arousal response during sleep. Following safe sleep guidelines is even more critical when a baby is ill.
Does inflammation always lead to SIDS?
No. Most infants experience inflammation from infections without any complications. SIDS only occurs when that inflammation interacts with a pre-existing biological vulnerability and a critical developmental window.
Why is stomach sleeping more dangerous during an infection?
Stomach sleeping can obstruct the airway. If an infant is already struggling with inflammation or congestion from a cold, their ability to overcome that obstruction is reduced. This combination significantly increases the risk of hypoxia.
Understanding the role of inflammation helps shift the conversation from “unpredictable death” to “identifiable biological risk.” While research continues into genetic markers for inflammation, adhering to safe sleep protocols remains the most effective way to protect infants during their most vulnerable months.