{kind=link}
Rectal ulceration can serve as an atypical, initial clinical manifestation of advanced HIV infection, often occurring in patients with severely compromised immune systems. When clinicians encounter persistent or painful perianal ulcerations, they should consider underlying HIV infection as a potential diagnosis, even in the absence of traditional respiratory or systemic symptoms.
Why Rectal Ulceration Occurs in Advanced HIV
Rectal ulceration in the context of HIV infection is frequently linked to profound immunosuppression, defined by a low CD4+ T-cell count. According to clinical data published in the Journal of the International Association of Providers of AIDS Care, opportunistic infections and malignancies are common drivers of anorectal pathology in patients with late-stage disease.
The mechanism involves the body’s inability to mount an effective localized immune response, allowing common pathogens—or rare opportunistic ones—to cause extensive tissue damage. Pathogens such as cytomegalovirus (CMV), herpes simplex virus (HSV), and syphilis are frequent culprits. In some instances, the ulceration is not caused by a secondary infection but by HIV-related lymphoproliferative disorders or direct mucosal involvement of the virus itself.
Clinical Presentation and Diagnosis
Patients presenting with rectal ulcers often report intense anorectal pain, rectal bleeding, or tenesmus—a persistent feeling of needing to evacuate the bowels. Because these symptoms mirror common conditions like hemorrhoids, fissures, or inflammatory bowel disease, the diagnosis of HIV is often delayed.
The standard diagnostic approach, as outlined by the Centers for Disease Control and Prevention (CDC), involves a comprehensive evaluation:
- Physical Examination: Careful inspection of the perianal area for characteristic lesions.
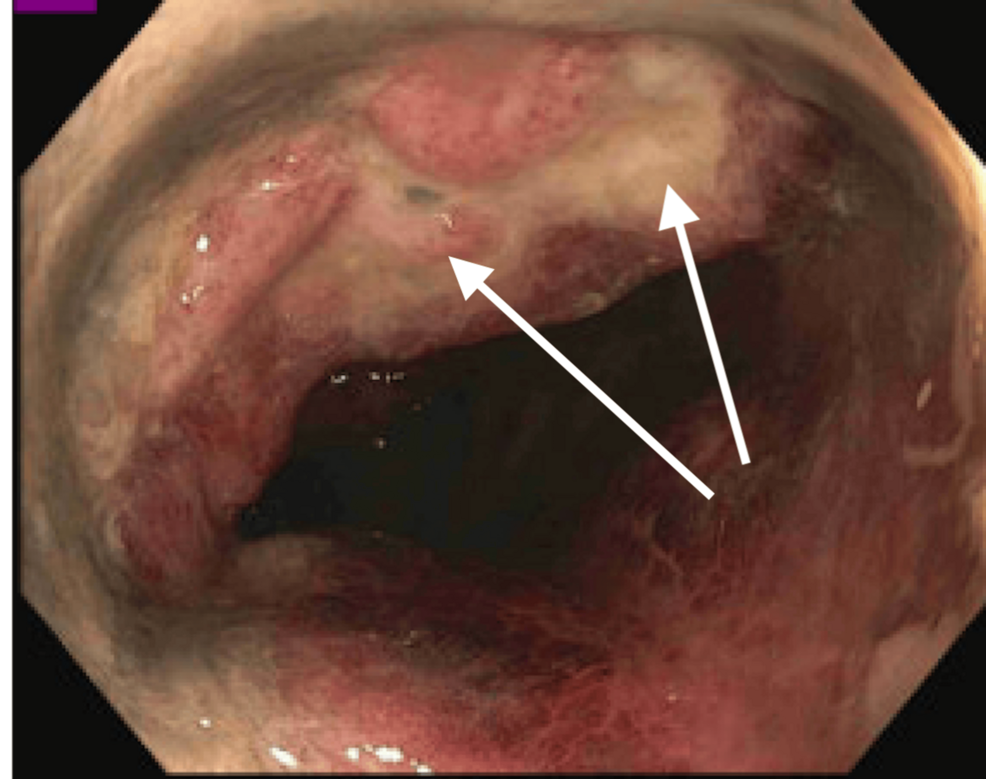
- Anoscopy or Proctoscopy: Direct visualization of the rectal mucosa to assess the depth and extent of the ulceration.
- Biopsy: Essential for ruling out malignancy and identifying causative pathogens via histopathology and immunohistochemistry.
- Serologic Testing: HIV screening is critical for any patient presenting with unexplained or non-healing anorectal ulcers.
The Importance of Early HIV Screening
The clinical significance of identifying HIV through an atypical presentation like a rectal ulcer cannot be overstated. Early diagnosis allows for the immediate initiation of antiretroviral therapy (ART). According to the National Institutes of Health (NIH), ART is the cornerstone of treatment, as it suppresses viral replication and allows for immune system reconstitution.

When a patient is diagnosed with HIV in an advanced state—often referred to as AIDS—the immediate clinical priority is to stabilize the patient while screening for other opportunistic infections. The resolution of rectal ulcerations typically correlates with the recovery of the patient’s CD4 count following the successful suppression of HIV viral load.
Comparison: Typical vs. Atypical HIV Manifestations
While most HIV diagnoses are prompted by generalized symptoms like persistent fever, weight loss, or lymphadenopathy, gastrointestinal manifestations provide a distinct diagnostic challenge.

| Feature | Typical Presentation | Atypical (Rectal) Presentation |
|---|---|---|
| Primary Symptoms | Fever, fatigue, weight loss | Anorectal pain, bleeding, ulcers |
| Diagnostic Pathway | Routine blood work | Anoscopy, biopsy, serology |
| Clinical Focus | Viral load management | Infection control, pain management, tissue biopsy |
When to Seek Medical Evaluation
Persistent anorectal symptoms that fail to respond to standard treatments for fissures or hemorrhoids warrant a clinical investigation for systemic conditions. Patients experiencing severe rectal pain, unexplained bleeding, or non-healing wounds in the perianal region should consult a healthcare provider. Clinicians are encouraged to maintain a high index of suspicion for HIV in these cases to ensure timely diagnosis and the prevention of further immune system decline.