{kind=link}
Breakthrough in IgG4-Related Disease: How Rituximab Is Changing Treatment for Tubulointerstitial Nephritis
Imagine battling a rare autoimmune disease that attacks your kidneys, only to face repeated relapses despite high-dose steroids. For patients with IgG4-related tubulointerstitial nephritis, this has been a frustrating reality—until now. A groundbreaking case study, published in the Journal of the American Society of Nephrology, reveals how rituximab, a targeted immunotherapy, is offering new hope as a steroid-sparing maintenance therapy for this challenging condition.
Here’s what you need to know about this medical breakthrough, its implications for patients, and what it means for the future of autoimmune kidney disease treatment.
What Is IgG4-Related Disease?
Immunoglobulin G4-related disease (IgG4-RD) is a systemic autoimmune disorder characterized by inflammation and fibrosis (scarring) in multiple organs. While it can affect nearly any part of the body—including the pancreas, salivary glands, and lymph nodes—its impact on the kidneys is particularly destructive. The most common renal manifestation is tubulointerstitial nephritis (TIN), a condition where the spaces between kidney tubules turn into inflamed, leading to:
- Progressive kidney damage
- Proteinuria (protein in urine)
- Hematuria (blood in urine)
- Declining kidney function (elevated serum creatinine)
- Hypocomplementemia (low levels of immune proteins)
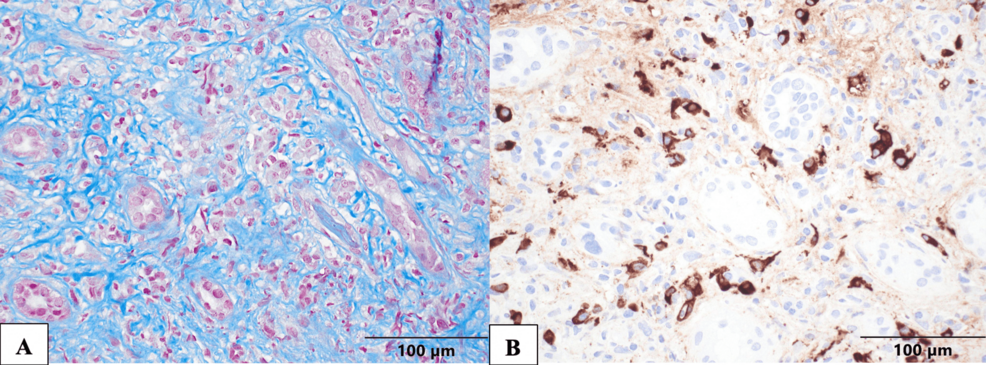
Diagnosis hinges on a kidney biopsy revealing dense lymphoplasmacytic infiltrates (immune cells flooding the tissue), storiform fibrosis (a swirling pattern of scar tissue), and an abundance of IgG4-positive plasma cells. While serum IgG4 levels are often elevated, they aren’t always a reliable marker—some patients test normal despite active disease.
The Problem With Traditional Treatment
For years, the standard treatment for IgG4-related TIN has been prolonged courses of glucocorticoids (e.g., prednisone). While steroids can reduce inflammation and improve kidney function initially, they come with significant drawbacks:
✔️ Benefits of Steroids
- Rapid reduction in inflammation
- Improvement in kidney function
- Widely available and inexpensive
❌ Risks of Long-Term Steroid Use
- Weight gain and metabolic syndrome
- Osteoporosis (bone thinning)
- Increased infection risk
- Diabetes and high blood pressure
- Mood swings and insomnia
- High relapse rates when tapering or discontinuing
Even more concerning? Some patients become refractory to steroids, meaning their disease flares up despite treatment. This was the case for a 58-year-old man described in a landmark 2015 case report published in Medicine (Baltimore). After multiple relapses and misdiagnoses (initially thought to be sarcoidosis), his kidney function continued to deteriorate—until a new approach changed everything.
Rituximab: A Game-Changer for Refractory Cases
Enter rituximab, a monoclonal antibody originally developed to treat certain cancers (like non-Hodgkin lymphoma) and autoimmune diseases (such as rheumatoid arthritis). It works by targeting CD20-positive B cells, a type of immune cell involved in IgG4-RD’s inflammatory cascade. The 2015 case report marked the first documented use of rituximab as a steroid-sparing therapy for IgG4-related TIN, with remarkable results:

The Patient’s Journey
- Initial Symptoms: Fatigue, 50-pound weight loss, shortness of breath, lymphadenopathy (swollen lymph nodes), and nephromegaly (enlarged kidneys).
- Misdiagnosis: Initially treated for chronic interstitial nephritis secondary to sarcoidosis with repeated prednisone courses.
- Breakthrough: A repeat kidney biopsy confirmed IgG4-related TIN.
- Treatment Shift: After failing to respond to steroids, the patient received rituximab.
- Outcome: Prompt and sustained improvement in kidney function. One year post-treatment, his serum creatinine stabilized, and imaging showed reduced kidney size.
This case demonstrated that rituximab could achieve remission where steroids failed, offering a lifeline for patients with refractory disease. But could it too prevent relapses?
Rituximab as Maintenance Therapy: The Latest Evidence
A 2024 study in the Journal of the American Society of Nephrology took rituximab’s role a step further, exploring its use as maintenance therapy to prevent relapses in IgG4-related TIN. The findings were promising:
- Reduced Relapse Rates: Patients on rituximab maintenance experienced fewer disease flares compared to those on steroids alone.
- Steroid-Sparing Effect: Many patients were able to taper or discontinue steroids entirely, reducing long-term side effects.
- Sustained Remission: Kidney function remained stable over extended follow-up periods.
This approach aligns with broader trends in autoimmune disease management, where targeted biologics are increasingly used to replace or supplement traditional immunosuppressants. For IgG4-RD, rituximab is emerging as a first-line option for patients who:
- Are refractory to steroids
- Experience frequent relapses
- Cannot tolerate long-term steroid side effects
How Rituximab Works in IgG4-Related Disease
To understand why rituximab is so effective, it helps to break down its mechanism of action:
- Targets B Cells: Rituximab binds to the CD20 protein on the surface of B cells, marking them for destruction by the immune system.
- Reduces IgG4 Production: By depleting B cells, rituximab lowers the production of IgG4 antibodies, which drive inflammation in IgG4-RD.
- Disrupts the Inflammatory Cycle: With fewer B cells, the cascade of immune responses that lead to fibrosis and organ damage is interrupted.
- Promotes Long-Term Remission: Unlike steroids, which only suppress symptoms temporarily, rituximab can induce deeper, more durable responses.
This targeted approach is a stark contrast to steroids, which broadly suppress the entire immune system, leading to widespread side effects.
Challenges and Considerations
While rituximab is a major advancement, it’s not without challenges:

1. Cost and Accessibility
Rituximab is significantly more expensive than steroids, which can limit access for some patients. Insurance coverage varies, and in some regions, it may not be readily available.
2. Side Effects
Though generally well-tolerated, rituximab can cause:
- Infusion reactions (fever, chills, nausea)
- Increased infection risk (due to B-cell depletion)
- Hypogammaglobulinemia (low antibody levels), which may require immunoglobulin replacement therapy
3. Long-Term Data
While early results are promising, long-term data on rituximab’s safety and efficacy in IgG4-RD are still emerging. Ongoing studies are needed to refine dosing strategies and identify which patients benefit most.
4. Not a Cure
Rituximab induces remission but doesn’t cure IgG4-RD. Some patients may require repeated courses or combination therapy with other immunosuppressants.
The Future of IgG4-Related Disease Treatment
The success of rituximab has opened the door to exploring other targeted therapies for IgG4-RD. Researchers are investigating:
- Other B-cell-targeted drugs: Such as obinutuzumab, which may offer improved efficacy with fewer side effects.
- Combination therapies: Pairing rituximab with other immunosuppressants to enhance remission rates.
- Biomarkers for personalized treatment: Identifying genetic or molecular markers to predict which patients will respond best to rituximab.
- Early intervention strategies: Using rituximab as a first-line therapy to prevent organ damage before it occurs.
As our understanding of IgG4-RD grows, so too does the potential for more effective, less toxic treatments. For patients who once faced a grim prognosis, these advances represent a beacon of hope.
Key Takeaways
- IgG4-related tubulointerstitial nephritis (TIN) is a rare but serious autoimmune kidney disease that can lead to progressive kidney damage.
- Traditional treatment with steroids is effective but comes with significant side effects and high relapse rates.
- Rituximab, a targeted B-cell therapy, has emerged as a steroid-sparing option for patients with refractory or relapsing disease.
- Recent studies reveal rituximab can induce sustained remission and reduce relapse rates when used as maintenance therapy.
- While promising, rituximab is not a cure and comes with its own challenges, including cost, side effects, and the need for long-term monitoring.
- The future of IgG4-RD treatment lies in personalized, targeted therapies that minimize side effects while maximizing efficacy.
Frequently Asked Questions
1. How is IgG4-related TIN diagnosed?
Diagnosis requires a kidney biopsy showing characteristic findings: dense lymphoplasmacytic infiltrates, storiform fibrosis, and IgG4-positive plasma cells. Serum IgG4 levels can be elevated but aren’t always reliable.
2. What are the symptoms of IgG4-related TIN?
Symptoms vary but often include:
- Fatigue and weight loss
- Swollen lymph nodes
- Enlarged kidneys (nephromegaly)
- Protein or blood in the urine
- Declining kidney function (elevated creatinine)
3. Who is at risk for IgG4-related disease?
IgG4-RD typically affects middle-aged to older adults, with a slight male predominance. It’s rare in children. The exact cause is unknown, but genetic and environmental factors may play a role.
4. Can IgG4-related TIN be cured?
Currently, there is no cure for IgG4-RD. However, treatments like rituximab can induce long-term remission, allowing patients to manage the disease effectively.
5. What other organs can IgG4-RD affect?
IgG4-RD is a multisystem disease that can involve:
- Pancreas (autoimmune pancreatitis)
- Salivary and lacrimal glands (Mikulicz’s disease)
- Lungs (IgG4-related lung disease)
- Aorta (IgG4-related aortitis)
- Lymph nodes (IgG4-related lymphadenopathy)
6. How is rituximab administered?
Rituximab is given as an intravenous infusion, typically in a hospital or clinic setting. The initial course usually involves two infusions two weeks apart, followed by maintenance doses every 6–12 months, depending on the patient’s response.
The Bottom Line
For patients with IgG4-related tubulointerstitial nephritis, the introduction of rituximab as a maintenance therapy marks a significant turning point. No longer are they limited to steroids alone—a treatment that, while effective, often comes with debilitating side effects and a high risk of relapse. With rituximab, there’s now a targeted, steroid-sparing option that can induce sustained remission and improve quality of life.
As research continues, the hope is that even more effective therapies will emerge, bringing us closer to a future where IgG4-RD is not just manageable, but curable. For now, patients and clinicians alike can take heart in knowing that progress is being made—one breakthrough at a time.
Worth a look