{kind=link}
Stroke-Induced Hydrocephalus: When a Brain Injury Triggers Unilateral Ventricular Enlargement
A stroke can leave behind a cascade of complications, some of which are life-altering. Among the most concerning is hydrocephalus—a condition characterized by an abnormal buildup of cerebrospinal fluid (CSF) in the brain’s ventricles. While hydrocephalus is often associated with congenital defects or aging, it can also develop after a stroke, particularly when it leads to unilateral ventricular enlargement (enlargement of just one ventricle).
This condition, though rare, demands urgent attention. If left untreated, it can cause irreversible brain damage, cognitive decline, and even death. In this article, we’ll break down:
- How strokes trigger hydrocephalus and unilateral ventricular enlargement
- The key symptoms and warning signs to watch for
- Diagnostic methods and why early detection is critical
- Treatment options, including surgical interventions
- Recovery outlook and long-term management strategies
How a Stroke Can Lead to Hydrocephalus
Hydrocephalus occurs when there’s a disruption in the flow or absorption of cerebrospinal fluid (CSF), the clear fluid that cushions the brain and spinal cord. Normally, CSF is produced in the ventricles, circulates through the brain, and is reabsorbed into the bloodstream. But after a stroke, several mechanisms can interfere with this delicate balance:
1. Obstructive Hydrocephalus: Blocked CSF Flow
Strokes often damage brain tissue, including areas that regulate CSF circulation. For example:
- Intracerebral hemorrhage (bleeding within the brain) can compress the aqueduct of Sylvius, the narrow channel connecting the third and fourth ventricles. This blockage prevents CSF from draining properly.
- Ischemic stroke (blocked blood flow) in the basal ganglia or thalamus may damage structures that control CSF absorption, leading to fluid buildup.
2. Communicating Hydrocephalus: Impaired Absorption
Even without a physical blockage, strokes can disrupt the brain’s ability to reabsorb CSF. The arachnoid granulations—tiny structures in the brain’s lining—are responsible for filtering CSF back into the blood. Stroke-induced inflammation or scarring can impair their function, causing fluid to accumulate in the ventricles.
3. Unilateral Ventricular Enlargement: Why One Side Swells
In most cases, hydrocephalus affects both ventricles symmetrically. However, unilateral ventricular enlargement (enlargement of just one ventricle) can occur due to:
- Asymmetric brain injury: A stroke on one hemisphere may cause localized swelling, compressing the adjacent ventricle and preventing CSF drainage on that side.
- Vascular compression: A hemorrhage or ischemic lesion near the foramen of Monro (the opening between the lateral and third ventricles) can obstruct CSF flow unilaterally.
- Post-stroke inflammation: Scar tissue formation (gliosis) may create a one-sided barrier, restricting fluid movement.
Key Insight: Unilateral hydrocephalus is often a secondary complication of stroke, meaning it develops after the initial brain injury—sometimes weeks or even months later. This delayed onset makes it particularly dangerous, as symptoms may be mistaken for stroke recovery or depression.
Recognizing the Warning Signs
Symptoms of stroke-induced hydrocephalus overlap with those of the original brain injury, making diagnosis challenging. However, certain red flags should trigger further evaluation:
Early Symptoms (Mild to Moderate Hydrocephalus)
- Cognitive decline: Memory loss, confusion, or difficulty concentrating (“pseudodementia”)
- Gait disturbances: Unsteady walking, frequent falls, or a shuffling gait
- Urinary incontinence: Loss of bladder control, often sudden
- Headaches: Worsening with coughing, straining, or lying down
Late Symptoms (Severe or Untreated Hydrocephalus)
- Severe cognitive impairment: Difficulty speaking, hallucinations, or personality changes
- Nausea and vomiting: Due to increased intracranial pressure
- Vision problems: Blurred or double vision (papilledema)
- Seizures: In advanced cases, as brain tissue becomes compressed
Why Symptoms Are Often Missed
Many of these signs (e.g., memory problems, gait issues) are attributed to:

- Normal aging
- Post-stroke recovery
- Depression or anxiety
This delay in diagnosis can lead to ventricular dilation, where the affected ventricle expands, increasing pressure on surrounding brain tissue.
Diagnosing Stroke-Related Hydrocephalus
Accurate diagnosis requires a combination of clinical evaluation and advanced imaging. Here’s how doctors confirm the condition:
1. Neurological Examination
A physician will assess:
- Mental status (memory, orientation, mood)
- Motor function (balance, coordination)
- Cranial nerve function (vision, eye movement)
2. Imaging Studies
The gold standard for diagnosing hydrocephalus is brain imaging, particularly:
- Computed Tomography (CT) Scan: Shows enlarged ventricles, signs of increased intracranial pressure, and any structural blockages. Example CT findings
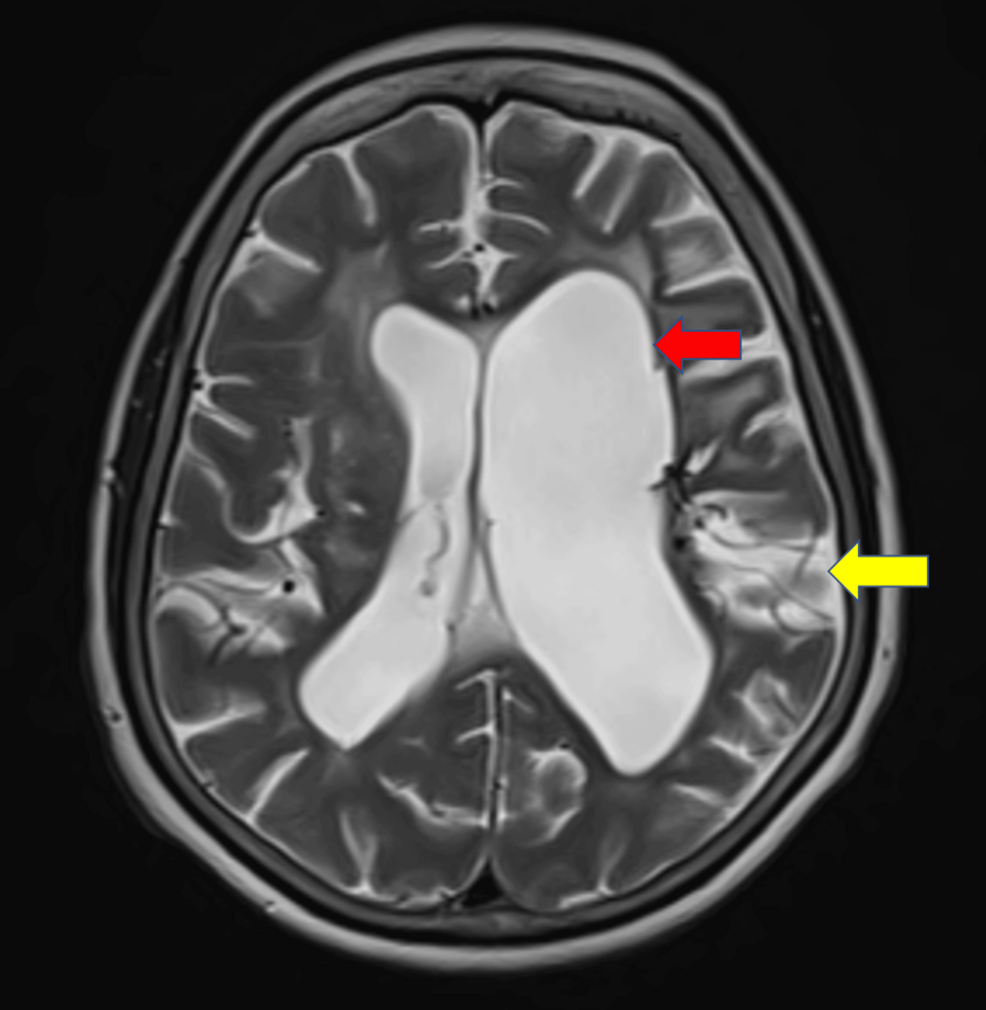
- Magnetic Resonance Imaging (MRI): Provides detailed images of CSF flow dynamics and can detect early changes in brain tissue. MRI characteristics of hydrocephalus
- CT or MRI with Contrast: Helps identify obstructions in the CSF pathways.
3. Specialized Tests
In some cases, additional tests may be needed:

- Transfontanellar ultrasound (for infants or patients with open fontanelles)
- CSF tap test: A small amount of CSF is removed to see if symptoms improve, confirming hydrocephalus.
- Intracranial pressure monitoring: For patients with unclear symptoms but suspected high pressure.
Diagnostic Challenge: Unilateral hydrocephalus can mimic other conditions, such as brain tumors or chronic subdural hematomas. A radiologist experienced in neuroimaging is crucial for accurate interpretation.
Treatment Options: From Medications to Surgery
Treatment depends on the severity of hydrocephalus and whether it’s obstructive or communicating. Options range from conservative management to life-saving surgery.
1. Conservative Management (Early or Mild Cases)
- Diuretics (e.g., acetazolamide): Reduce CSF production to temporarily ease pressure.
- Steroids (e.g., dexamethasone): Decrease inflammation around blocked CSF pathways.
- Monitoring: Frequent neurological exams to track progression.
Limitation: These treatments address symptoms but do not resolve the underlying blockage or absorption issue.
2. Endoscopic Third Ventriculostomy (ETV)
A minimally invasive procedure where a neurosurgeon creates a new opening in the third ventricle to allow CSF to bypass the blockage. This is often the first-line surgical option for obstructive hydrocephalus.
- Success rate: ~60–80% for long-term relief
- Recovery time: 1–3 days in hospital
- Risks: Infection, bleeding, or persistent CSF leakage
3. Ventriculoperitoneal (VP) Shunt
If ETV fails or the hydrocephalus is communicating, a VP shunt may be necessary. This involves inserting a tube to drain excess CSF from the ventricle into the abdomen, where it’s absorbed.
- Effectiveness: ~90% success rate, but requires lifelong management
- Complications: Shunt failure (20–30% within 5 years), infection, or abdominal discomfort
4. Treatment for Unilateral Hydrocephalus
When only one ventricle is enlarged, options include:
- Asymmetrical shunt placement: Draining only the affected ventricle.
- Endoscopic fenestration: Creating a connection between the enlarged and normal ventricle to balance pressure.
- Surgical resection: Removing scar tissue or lesions compressing the ventricle (e.g., after a hemorrhagic stroke).
Note: Unilateral hydrocephalus often requires a customized approach, as standard treatments may not be effective.
Recovery and Long-Term Outlook
The prognosis for stroke-induced hydrocephalus depends on:
- Timeliness of diagnosis and treatment
- Underlying cause (e.g., ischemic vs. Hemorrhagic stroke)
- Patient’s overall health and age
Short-Term Recovery (First 6–12 Months)
- Improved cognition: Memory and concentration may return within weeks of effective treatment.
- Stabilized gait: Balance often improves as CSF pressure normalizes.
- Reduced headaches: Many patients report relief after shunt placement or ETV.
Long-Term Management
Even after successful treatment, some patients require ongoing care:
- Shunt maintenance: Regular check-ups to monitor for blockages or infections.
- Physical therapy: To regain strength and coordination.
- Neuropsychological support: Cognitive rehabilitation for memory or executive function deficits.
When to Seek Emergency Care
Contact a doctor immediately if you or a loved one experience:
- Sudden severe headache
- Confusion or inability to wake up
- Seizures
- Loss of vision or slurred speech
These could indicate acute hydrocephalus, a medical emergency requiring urgent drainage.
Hopeful Note: While stroke-induced hydrocephalus is serious, early intervention can prevent permanent damage. Advances in neuroimaging and minimally invasive surgery have improved outcomes significantly in recent years.
Frequently Asked Questions
1. Can hydrocephalus develop years after a stroke?
Yes. In some cases, delayed hydrocephalus can emerge months or even years after the initial stroke due to gradual scar tissue formation or delayed CSF absorption issues.

2. Is unilateral hydrocephalus more dangerous than bilateral?
Not necessarily in terms of immediate risk, but unilateral hydrocephalus is often harder to diagnose because symptoms may be subtle. The danger lies in delayed treatment, which can lead to irreversible damage on the affected side.
3. Are there non-surgical treatments for hydrocephalus?
Non-surgical options (e.g., diuretics, steroids) can help manage symptoms temporarily, but they do not resolve the underlying blockage or absorption problem. Surgery remains the definitive treatment for most cases.
4. How common is hydrocephalus after a stroke?
Studies suggest hydrocephalus occurs in 5–10% of stroke patients, with higher rates in those who experience intracerebral hemorrhage. Unilateral ventricular enlargement is rarer, affecting 1–3% of stroke survivors.
Source: Stroke and Hydrocephalus (Neurology Journal)
5. Can hydrocephalus be prevented after a stroke?
There’s no guaranteed way to prevent hydrocephalus, but aggressive blood pressure control, antiplatelet therapy (for ischemic strokes), and prompt treatment of hemorrhages can reduce the risk of complications like CSF blockages.
Key Takeaways
- Stroke-induced hydrocephalus occurs when brain injury disrupts CSF flow or absorption, leading to fluid buildup in the ventricles.
- Unilateral ventricular enlargement is a rare but serious variant where only one ventricle swells, often due to localized stroke damage.
- Symptoms like memory loss, gait problems, and incontinence (the “wet, wacky, wobbly” triad) may be mistaken for aging or recovery.
- Diagnosis requires CT/MRI scans and neurological exams; delay can worsen outcomes.
- Treatment ranges from medications to endoscopic surgery or VP shunts, with unilateral cases needing specialized approaches.
- Early intervention improves recovery, but lifelong monitoring is often necessary for shunt-dependent patients.
When to Act: Seek Help Now
If you or a loved one has experienced a stroke and notice any of the following, consult a neurologist immediately:
- Progressive confusion or memory loss
- Difficulty walking without assistance
- Severe, persistent headaches
- Bladder control issues
Hydrocephalus is treatable, but time is brain. Don’t wait—early diagnosis saves lives and preserves cognitive function.