{kind=link}
Understanding Autoimmune Pancreatitis: Types, Diagnosis, and Treatment
Autoimmune pancreatitis (AIP) is a rare fibroinflammatory subtype of chronic pancreatitis caused by aberrant immune responses. Because its symptoms and imaging often mimic pancreatic cancer, it presents a significant diagnostic challenge for clinicians. However, unlike malignancy, AIP is highly responsive to medical therapy, making an accurate diagnosis critical for patient outcomes.
Key Takeaways
- AIP is categorized into two primary forms: Type 1 and Type 2.
- Type 1 is associated with IgG4-related disease and typically affects older males.
- Type 2 is less frequent, often affects younger individuals, and is confined to the pancreas.
- Glucocorticoid steroid treatment leads to clinical remission in nearly 100% of cases for both types.
The Two Types of Autoimmune Pancreatitis
Medical professionals distinguish between two distinct forms of the disease, which differ in their systemic involvement and patient demographics.
Type 1 AIP (T1-AIP)
Type 1 AIP, also known as lymphoplasmacytic sclerosing pancreatitis, is recognized as the pancreatic manifestation of immunoglobulin 4 (IgG4)-related disease. It commonly appears in individuals in their seventh decade of life and shows a considerable male predominance. This type is frequently associated with elevated serum IgG4 levels and the presence of IgG4-positive cells on tissue biopsies.
Type 2 AIP
Type 2 AIP is also referred to as idiopathic duct-centric chronic pancreatitis. Unlike Type 1, Type 2 is confined to the pancreas and does not involve other organs. It is less frequent than Type 1 and typically affects younger individuals. It is also associated with inflammatory processes.
Diagnostic Challenges and Clinical Presentation
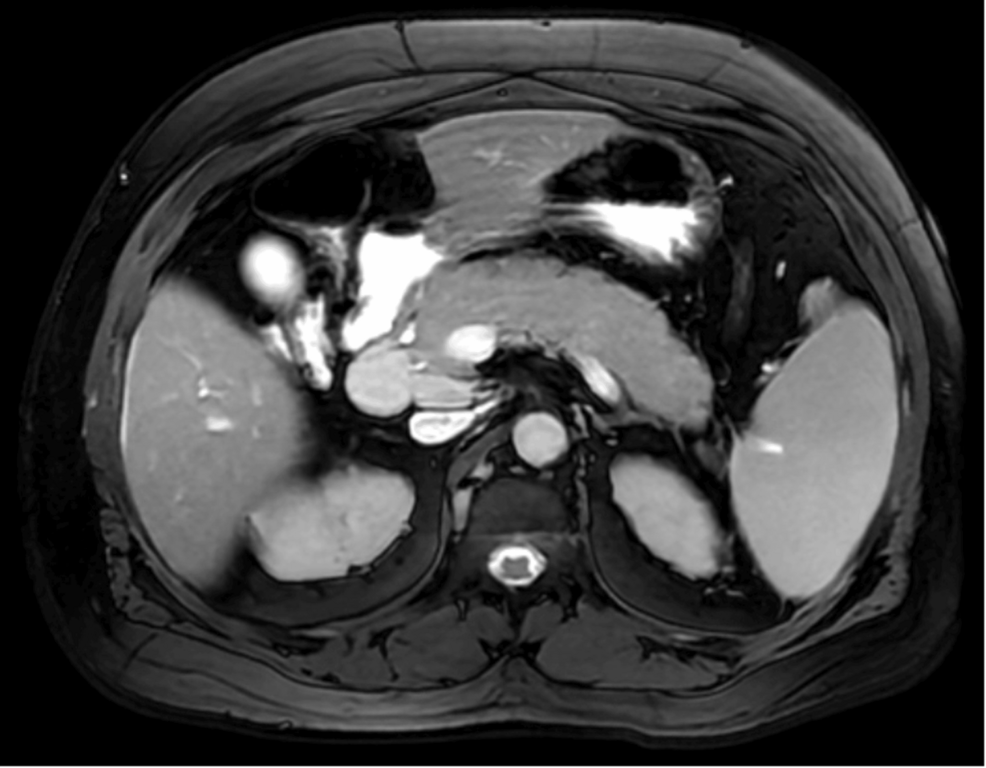
Diagnosing AIP can be difficult because it often presents as a mass on imaging, which can be easily mistaken for pancreatic adenocarcinoma. Common presentations include:
- Multifocal Masses: In some rare cases, AIP may present as multiple masses within the pancreas.
- Painless Jaundice: Patients may experience progressive, painless jaundice due to the inflammation affecting the bile ducts.
- Incidental Findings: Some patients are diagnosed after a CT scan reveals a mass in the pancreatic head or tail during an evaluation for other issues.
To rule out malignancy, doctors may use a combination of serum IgG4 testing, CT imaging, and pancreatic biopsies.
Treatment and Prognosis
The primary treatment for both Type 1 and Type 2 autoimmune pancreatitis is the administration of glucocorticoid steroids. This therapy is highly effective, leading to clinical remission in almost 100% of cases for both types. The goal of treatment is to reduce inflammation and resolve the masses or obstructions caused by the immune response.
Frequently Asked Questions
How does AIP differ from pancreatic cancer?
Even as both can appear as masses on a CT scan, AIP is an inflammatory condition that responds rapidly to steroids, whereas pancreatic cancer is a malignancy that requires surgical or oncological intervention. Diagnosis often requires biopsy or blood tests for IgG4.

Who is most likely to develop Type 1 AIP?
Type 1 AIP most commonly affects men in their 60s and is linked to a broader systemic disease involving IgG4.
Is Type 2 AIP a systemic disease?
No, Type 2 AIP is confined to the pancreas, whereas Type 1 can be part of a systemic IgG4-related disease affecting other organs.
Summary
Autoimmune pancreatitis is a complex condition that requires careful differentiation from pancreatic cancer to avoid unnecessary surgical interventions. Whether presenting as a single mass or multifocal lesions, the disease is characterized by a strong response to steroid therapy. As diagnostic tools and the understanding of IgG4-related diseases evolve, the ability to achieve rapid clinical remission continues to improve.