{kind=link}
Laparoscopic Management of Spontaneous Heterotopic Pregnancy With Preservation of Intrauterine Pregnancy
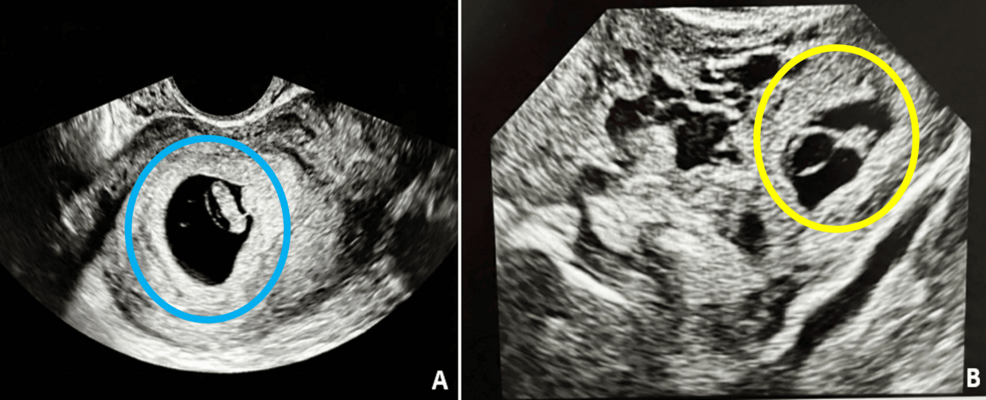
Heterotopic pregnancy is a rare but potentially life-threatening condition in which an intrauterine pregnancy coexists with an ectopic pregnancy. Though uncommon, its incidence has risen with the increased use of assisted reproductive technologies. Early diagnosis is challenging because symptoms may be absent or masked by the presence of a viable intrauterine pregnancy, leading to delayed intervention and increased risk of rupture.
Laparoscopy is the preferred surgical approach for managing heterotopic pregnancy in hemodynamically stable patients. This minimally invasive technique allows for precise removal of the ectopic gestation whereas preserving the intrauterine pregnancy when feasible. In a reported case, a 37-year-old G1P0 woman at 11 weeks and 5 days gestation presented for a routine ultrasound when signs of heterotopic pregnancy were noted. She was asymptomatic, with no abdominal pain or vaginal bleeding. Her history included hypothyroidism following thyroidectomy for papillary thyroid cancer and essential hypertension.
After consultation with interventional radiology for backup, the patient underwent laparoscopic unilateral salpingo-oophorectomy with removal of the abdominal pregnancy. Pathological examination confirmed a secondary abdominal pregnancy. The intrauterine pregnancy was preserved, and the patient went on to carry it to term. At 38 weeks and 3 days, she was induced due to chronic hypertension and delivered vaginally without complications. The newborn weighed 3800 grams with Apgar scores of 8 and 9. Ectopic placental tissue regressed postpartum without further intervention.
This case underscores the importance of maintaining a high index of suspicion for heterotopic pregnancy even after confirming an intrauterine gestation. A systematic approach, including careful adnexal examination during ultrasound, is essential for early detection. When diagnosed, laparoscopic management offers a safe and effective means of resolving the ectopic component while supporting the continuation of the uterine pregnancy, ultimately improving maternal and fetal outcomes.
Key Takeaways
- Heterotopic pregnancy involves a concurrent intrauterine and ectopic pregnancy and is considered a medical emergency if undiagnosed.
- Laparoscopy is the standard of care for hemodynamically stable patients, allowing removal of the ectopic gestation with minimal invasiveness.
- In select cases, the intrauterine pregnancy can be preserved and carried to term with favorable outcomes.
- Asymptomatic presentation does not rule out heterotopic pregnancy; vigilance during early prenatal imaging is critical.
- Postpartum regression of ectopic placental tissue can occur, reducing the need for additional treatment.
Frequently Asked Questions
What is a heterotopic pregnancy?
A heterotopic pregnancy is a rare condition in which a woman has both an intrauterine pregnancy (inside the uterus) and an ectopic pregnancy (outside the uterus, such as in the fallopian tube, abdomen, or cervix) at the same time.
Why is heterotopic pregnancy tricky to diagnose?
Diagnosis is challenging because the presence of a normal intrauterine pregnancy may lead clinicians to overlook the possibility of an ectopic gestation. Many patients are asymptomatic in the early stages, delaying clinical suspicion.
Is laparoscopic surgery safe for treating heterotopic pregnancy?
Yes, laparoscopy is the preferred surgical method for hemodynamically stable patients with heterotopic pregnancy. It allows for precise removal of the ectopic tissue while minimizing trauma and preserving the intrauterine pregnancy when possible.
Can a woman have a normal vaginal delivery after laparoscopic management of heterotopic pregnancy?
Yes, as demonstrated in clinical cases, women can go on to have uncomplicated vaginal deliveries at term following laparoscopic intervention, with healthy neonatal outcomes.
What happens to the ectopic placental tissue after treatment?
In some cases, the ectopic placental tissue undergoes spontaneous regression after delivery or surgical removal, eliminating the need for further intervention.