{kind=link}
Advancements in Gene Therapy for Congenital Deafness: Sequential Bilateral Treatment
Recent clinical progress in gene therapy for genetic hearing loss demonstrates that sequential bilateral treatment is both safe and effective, according to research published in Nature Medicine. By leveraging the immune-privileged environment of the inner ear, researchers have successfully delivered restorative gene therapies to both ears in patients with congenital deafness, marking a significant step forward in treating hereditary hearing impairment.
Understanding Gene Therapy for Congenital Deafness
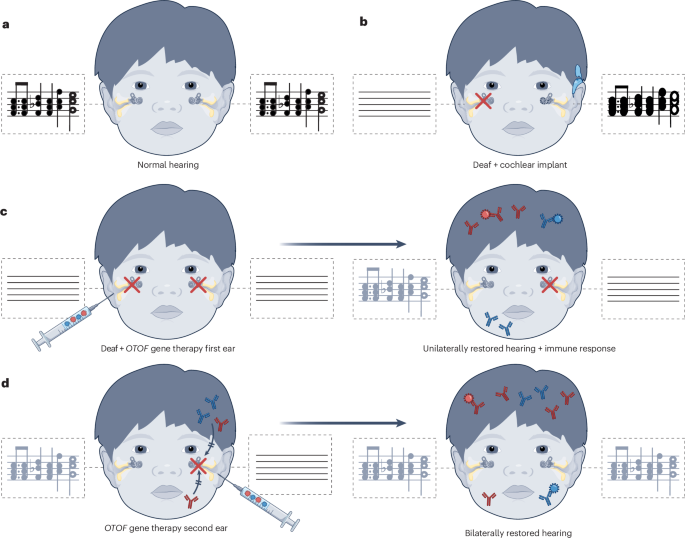
Congenital deafness often results from mutations in specific genes, such as the OTOF gene, which encodes otoferlin, a protein essential for the transmission of sound signals from the inner ear to the auditory nerve. Gene therapy aims to address these conditions by delivering a functional copy of the gene directly into the sensory cells of the cochlea.
The primary challenge in bilateral treatment—treating both ears—has historically been the risk of an immune response. If the body detects the viral vector used to deliver the gene therapy in the first ear, it may develop antibodies that neutralize the treatment when it is administered to the second ear. However, the inner ear is recognized as an “immune-privileged” site, meaning it has unique mechanisms to limit inflammation and immune cell infiltration. Recent data confirms that this environment allows for successful sequential delivery without triggering a systemic immune rejection that would negate the second procedure’s benefits.
Clinical Feasibility and Safety Profiles
The safety of sequential bilateral administration relies on the localized nature of the gene delivery. According to the Nature Medicine findings, the surgical approach involves a precise injection into the cochlea, which minimizes exposure to the bloodstream.
* Immune Privilege: The blood-labyrinth barrier effectively isolates the inner ear, preventing the immune system from identifying the viral vector as a threat after the first dose.
* Sequential Timing: Clinical protocols suggest that spacing the procedures allows for the stabilization of the first ear while maintaining the therapeutic window for the second.
* Efficacy: Patients receiving sequential treatment have shown measurable improvements in auditory brainstem response (ABR) and speech perception tests, confirming that the restored proteins function correctly in both cochleae.
Comparison with Unilateral Treatment
Historically, clinical trials for hearing loss gene therapy focused on unilateral treatment—treating only one ear—to minimize risk. This approach provided proof of concept but left patients with asymmetric hearing restoration.
| Feature | Unilateral Gene Therapy | Sequential Bilateral Therapy |
| :— | :— | :— |
| Primary Goal | Proof of safety and efficacy | Restoration of binaural hearing |
| Risk Profile | Low systemic exposure | Minimal systemic exposure due to immune privilege |
| Auditory Outcome | Improved hearing in one ear | Improved localization and speech in noise |
Binaural hearing is critical for sound localization and understanding speech in noisy environments. The ability to safely treat both ears represents a move toward restoring natural hearing function rather than providing partial compensation.
Future Directions in Auditory Medicine
The success of these trials opens the door for broader applications of gene therapy in other forms of hereditary deafness. As researchers refine the viral vectors and delivery techniques, the focus is shifting toward long-term durability and the potential for treating adult-onset genetic hearing loss.
Regulatory bodies, including the FDA and the European Medicines Agency (EMA), continue to monitor these developments as they transition from early-phase clinical trials to broader therapeutic applications. Future studies are expected to refine the ideal age for intervention, as early treatment remains a priority for maximizing the development of the auditory cortex in pediatric patients.
Worth a look