{kind=link}
Restoring Hand Function: Breakthrough Brain-Computer Interface Study
A recent clinical study demonstrates that a dual-interface system—combining an implanted brain-computer interface (BCI) with spinal cord stimulation—can restore voluntary hand and arm movement in a patient with chronic tetraplegia.
The Mechanism of Neural Decoding and Stimulation
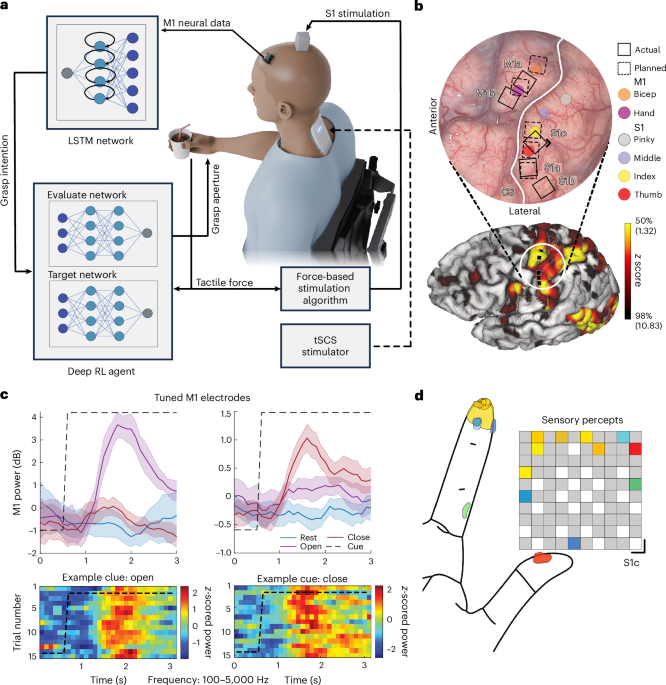
The study, registered at ClinicalTrials.gov (NCT03680872), involved a 42-year-old male participant who sustained a C4 sensory/C5 motor spinal cord injury (ASIA Impairment Scale A) in 2020. Researchers implanted microelectrode arrays into the participant’s motor cortex (M1) and somatosensory cortex (S1).
When the participant imagines moving his hand, the implanted arrays record these electrical signals. A computer processor then translates these intentions into digital commands.
Restoring Sensory Feedback
A significant innovation in this research is the integration of closed-loop sensory feedback. While traditional BCIs focus solely on motor output, this system utilizes the S1 implants to provide the user with a sense of touch. S1-ICMS through SIROF microelectrode arrays generated percepts at the fingertips of the participant.
Clinical Significance of Combined Therapies
The research team employed a multimodal approach, pairing the BCI with transcutaneous spinal cord stimulation (tSCS). This non-invasive stimulation primes the spinal cord, lowering the threshold for muscle recruitment and enhancing the effectiveness of the implanted device. By combining cortical control with spinal-level stimulation, the participant achieved functional gains. The study protocol was conducted under an Investigational Device Exemption (IDE G170200) granted by the U.S. Food and Drug Administration (FDA).
Key Takeaways for Neuro-Rehabilitation
- Bidirectional Control: The system bridges the gap between the brain and the muscles, enabling both motor execution and sensory perception.
- Functional Autonomy: The participant moved from requiring complete assistance with activities of daily living (ADLs) to performing self-directed grasping and reaching tasks.
- Surgical Precision: Implantation was guided by functional MRI (fMRI) and intraoperative mapping to ensure the electrodes were placed in the cortical areas corresponding to hand and finger movement.
Future Directions
Worth a look