{kind=link}
The Hidden Toll: Understanding Collateral Mortality After the Pandemic
When we discuss the impact of the COVID-19 pandemic, the conversation usually centers on the virus itself. However, a more complex and quieter crisis emerged alongside the infection rates: collateral mortality. This refers to the increase in deaths from non-COVID causes, driven by the systemic collapse of healthcare access, delayed screenings, and the psychological toll of global lockdowns.
For many, the pandemic didn’t just bring a new virus; it created a barrier between patients and the life-saving care they already needed. Understanding this shift is critical for rebuilding health systems that are resilient enough to handle both a primary crisis and the secondary health failures that follow.
- Indirect Deaths: Collateral mortality includes deaths from heart disease, stroke, and cancer that occurred because patients couldn’t or wouldn’t seek care.
- Systemic Barriers: Hospital redirections, staffing shortages, and fear of infection led to a significant drop in preventative screenings.
- The “Scarring” Effect: Some health declines triggered during the pandemic have created long-term chronic issues that persist years later.
- Equity Gap: Marginalized populations suffered disproportionately due to lack of telehealth access and existing healthcare disparities.
What Exactly is Collateral Mortality?
Collateral mortality, often categorized under excess mortality
, represents the difference between the observed number of deaths in a population and the number of deaths expected based on historical trends. While direct mortality is caused by the virus, collateral mortality is the result of the environment the virus created.
This phenomenon occurs through several distinct channels. First, there is the displacement of care, where hospitals prioritized COVID-19 patients, leading to the cancellation of elective surgeries and routine check-ups. Second, there is patient avoidance, where individuals avoided clinics for fear of contracting the virus, often ignoring early warning signs of serious illness.
The Primary Drivers of Non-COVID Deaths
1. Cardiovascular Crisis
Heart disease and stroke saw a marked increase in mortality during the pandemic. According to research published in eLife, the disruption in emergency care for acute myocardial infarctions (heart attacks) contributed to a rise in indirect deaths. When people stopped calling emergency services for chest pain, they missed the critical window for intervention, leading to higher rates of permanent heart damage or death.
2. The Cancer Screening Gap
Preventative screenings for colorectal, breast, and cervical cancers plummeted during the height of the pandemic. This didn’t necessarily cause an immediate spike in deaths, but it created a “stage-shift.” This means cancers that would have been caught at Stage I or II were instead diagnosed at Stage III or IV, significantly reducing the chances of successful treatment.
3. Mental Health and Substance Abuse
The isolation of lockdowns and the stress of economic instability triggered a surge in “deaths of despair.” This includes an increase in opioid overdoses and suicides. The loss of community support systems and the disruption of outpatient mental health services left millions vulnerable without a safety net.
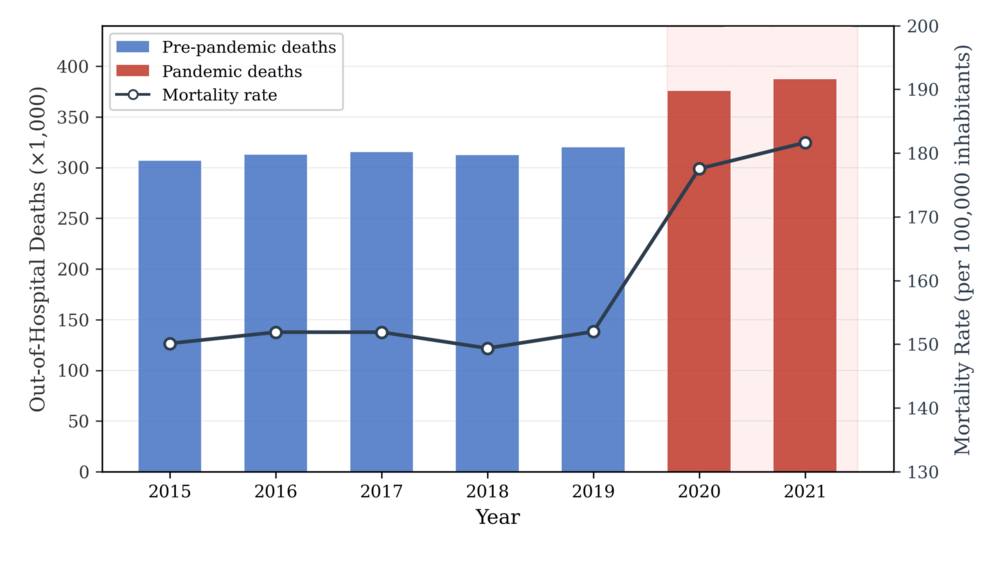
The Impact Outside Hospital Walls
While much of the data focuses on clinical settings, the collateral damage extended deep into the community. The disruption of primary care—the first line of defense in health—meant that manageable conditions like hypertension and diabetes went unmonitored. This led to a higher frequency of preventable complications that eventually required hospitalization, further straining an already exhausted system.
“Excess mortality studies provide crucial information regarding the health burden of pandemics and other large-scale events,” helping researchers separate the direct contribution of a virus from the indirect consequences of the societal response. eLife Research Analysis
Addressing the Long-Term “Scarring” Effect
Public health experts now warn of a “scarring” effect. This occurs when a temporary disruption in care leads to a permanent decline in health. For example, a patient who missed two years of dialysis or blood pressure management may now have chronic kidney disease or heart failure that cannot be fully reversed, even though healthcare services have returned to normal.
How to Recover the Lost Ground
- Aggressive Screening Campaigns: Implementing “catch-up” programs for cancer screenings to identify late-stage diagnoses early.
- Expanding Telehealth: Using the digital infrastructure built during the pandemic to reach rural and underserved populations who previously lacked access.
- Integrated Behavioral Health: Embedding mental health services within primary care to address the lingering psychological effects of the pandemic.
Frequently Asked Questions
Did the lockdowns cause more deaths than the virus?
In most regions, direct COVID-19 deaths remained the primary driver of excess mortality. However, the percentage of indirect deaths varied by country and demographic, with some populations seeing a significant rise in non-COVID mortality due to healthcare collapse.

Why is this called “collateral” damage?
It is termed collateral because these deaths were not caused by the biological agent (the virus) but by the secondary effects of the pandemic, such as policy decisions, healthcare system failures, and societal fear.
How can I tell if I have a “pandemic gap” in my health?
If you missed any routine screenings, annual physicals, or specialist appointments between 2020 and 2023, you should contact your primary care provider to schedule a comprehensive wellness check, even if you perceive healthy.
Looking Ahead: Building a Resilient Future
The lesson of collateral mortality is clear: a health system that only prepares for the “headline” crisis is a system that fails its patients. Future pandemic preparedness must include “continuity of care” protocols—strategies that ensure cancer screenings, maternal health, and chronic disease management continue even when hospitals are under extreme pressure.
As we move forward, the goal is not just to recover from the pandemic, but to build a healthcare infrastructure that treats preventative care as an essential service, not an optional luxury.