{kind=link}
COVID-19 May Leave Placental Damage, But Virus Disappears After Maternal Recovery
Pregnant women infected with SARS-CoV-2 face heightened risks of severe illness, and emerging research shows that while the virus itself does not persist in the placenta after maternal recovery, it can cause lasting placental damage that affects fetal development. This damage, driven by maternal inflammation rather than direct viral invasion, is increasingly recognized as a key factor in adverse pregnancy outcomes such as intrauterine growth restriction (IUGR). Understanding the mechanisms behind placental injury and the protective roles of vaccination and anticoagulant therapy is critical for improving maternal and fetal health during the pandemic.
SARS-CoV-2 Does Not Persist in the Placenta After Maternal Recovery
Despite concerns about vertical transmission, multiple studies have confirmed that SARS-CoV-2 does not linger in placental tissue following maternal recovery from COVID-19. Research using placental models and clinical samples has consistently failed to detect persistent viral RNA or protein in the placenta after the acute infection phase. This indicates that while the virus can infect placental cells during active illness, it is cleared from the tissue as the mother’s immune response resolves.
This finding is significant due to the fact that it rules out long-term viral reservoirs in the placenta as a mechanism for ongoing fetal harm. Instead, the focus shifts to the indirect consequences of maternal infection—particularly the inflammatory response—as the primary driver of placental dysfunction.
Placental Inflammation Drives Fetal Complications
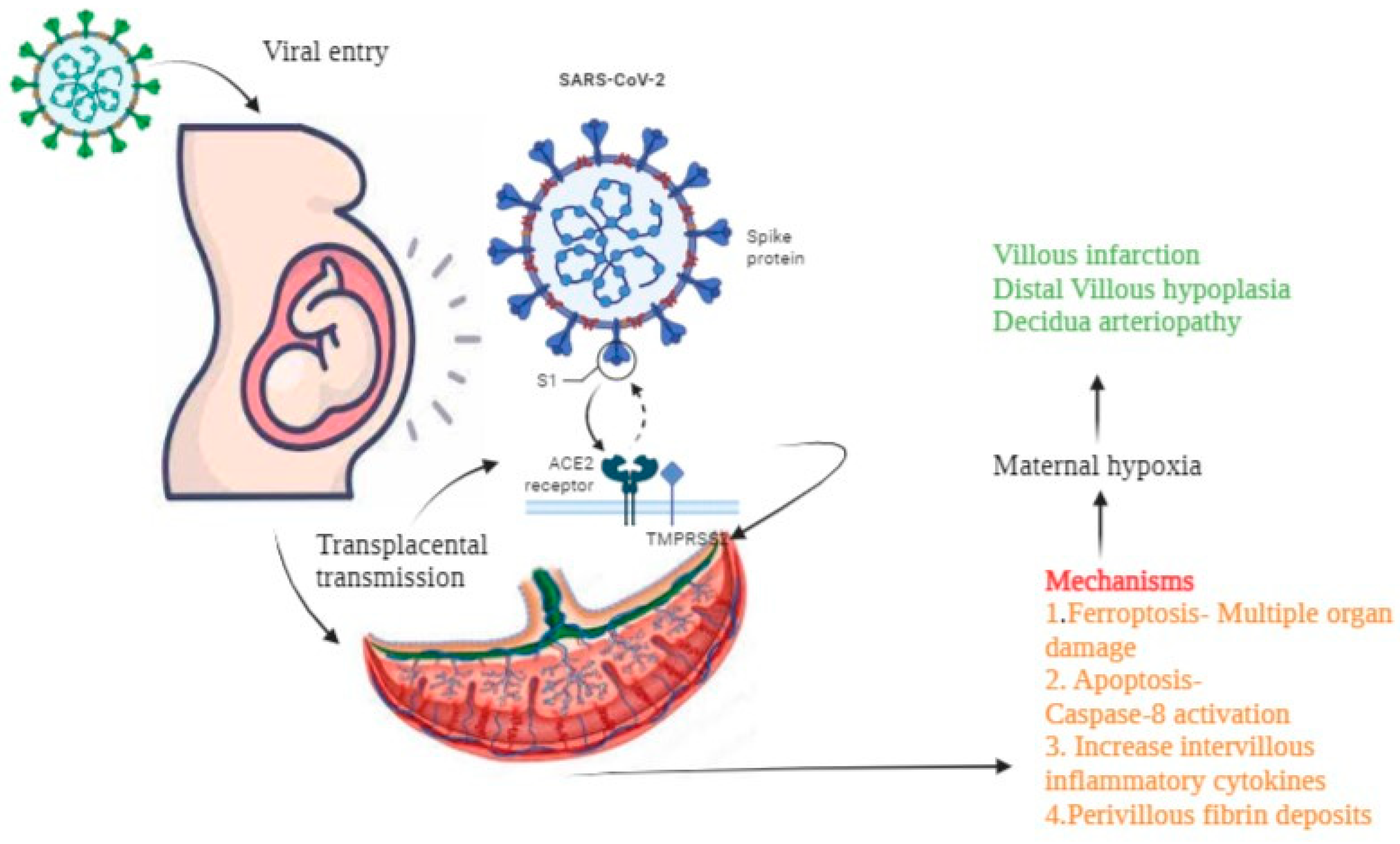
Although the virus clears, maternal SARS-CoV-2 infection triggers a robust inflammatory response that can damage the placenta. Studies in both human and animal models have shown that COVID-19 during pregnancy leads to placental pathology characterized by fibrin deposition, thrombosis, and elevated expression of inflammatory markers such as IP10, IL6, and IL10. These changes impair placental function and reduce nutrient and oxygen transfer to the fetus.
In a pregnant female hamster model of SARS-CoV-2 infection, researchers observed significant increases in IUGR despite the absence of vertical transmission. The growth restriction was directly linked to placental damage rather than fetal infection. Histological examination revealed widespread vascular injury and inflammatory cell infiltration in the placenta, which correlated with poor fetal outcomes.
These findings are consistent with human studies showing that pregnant women with severe or even mild COVID-19 are at increased risk of delivering babies with low birth weight or signs of fetal distress, even when the virus is not detected in fetal tissues.
Vaccination and Anticoagulant Therapy Protect the Placenta
Encouragingly, interventions that modulate the maternal immune response or prevent clotting can mitigate placental damage. Vaccination against SARS-CoV-2 has been shown to enhance viral clearance, reduce the severity of maternal illness, and lower placental inflammation. In animal models, vaccinated dams exhibited less placental injury and improved fetal growth compared to unvaccinated infected controls.
Similarly, anticoagulant therapy—specifically low-molecular-weight heparin such as enoxaparin—has demonstrated protective effects. In preclinical studies, enoxaparin treatment reduced fibrin deposition and thrombosis in the placenta, thereby preserving placental function and improving fetal outcomes. These results suggest that targeting the coagulopathic and inflammatory consequences of maternal infection may be a viable strategy to safeguard pregnancy.
Clinical Implications and Ongoing Research
The recognition of placental inflammation as a central mechanism of fetal harm in maternal COVID-19 has important clinical implications. It supports the prioritization of pregnant individuals for COVID-19 vaccination and reinforces the necessitate for close monitoring of fetal growth in pregnancies affected by SARS-CoV-2 infection, even in cases of mild or asymptomatic maternal disease.
Ongoing research continues to refine our understanding of the timing and severity of placental injury, as well as the potential benefits of early intervention. Long-term follow-up of infants born to mothers who had COVID-19 during pregnancy is also underway to assess any lasting neurodevelopmental or metabolic effects that may stem from altered intrauterine conditions.
As of April 2022, the accumulating evidence underscores a critical insight: while SARS-CoV-2 may not persist in the placenta, its impact on maternal immunity can leave a lasting imprint on placental health—one that directly influences the well-being of the next generation.
Key Takeaways
- SARS-CoV-2 does not persist in the placenta after maternal recovery from COVID-19.
- Placental damage from maternal infection is driven by inflammation, not direct viral persistence.
- This damage is characterized by fibrin deposition, thrombosis, and elevated inflammatory markers.
- Placental injury is a major contributor to intrauterine growth restriction (IUGR), even without vertical transmission.
- Vaccination enhances viral clearance and reduces placental inflammation.
- Anticoagulant therapy (e.g., enoxaparin) can mitigate placental thrombosis and improve fetal outcomes.
- Protecting maternal health through vaccination and timely intervention helps safeguard fetal development.
Worth a look