{kind=link}
Advancements in Deep Brain Stimulation for Parkinson’s Disease Gait Disorders
Deep brain stimulation (DBS) is a surgical treatment for Parkinson’s disease that, while highly effective for tremors and rigidity, often presents challenges in managing gait disturbances and freezing of gait (FOG). Recent clinical research indicates that adaptive DBS (aDBS) and frequency-tuned stimulation parameters are evolving to provide more precise control over these motor symptoms by targeting specific neural oscillations associated with movement.
How Does Deep Brain Stimulation Affect Parkinsonian Gait?
Traditional DBS of the subthalamic nucleus (STN) delivers continuous electrical stimulation to regulate basal ganglia activity. According to research published in Neurology, while this approach effectively reduces bradykinesia, its long-term impact on balance and gait remains variable. Studies suggest that while some patients experience improved stride length, others may see little change or, in rare cases, postoperative gait deterioration. This variability occurs because gait is a complex, multi-network process that involves not just the STN, but also the pedunculopontine nucleus (PPN) and cortical motor circuits.
Why Is Adaptive DBS Considered a Breakthrough?
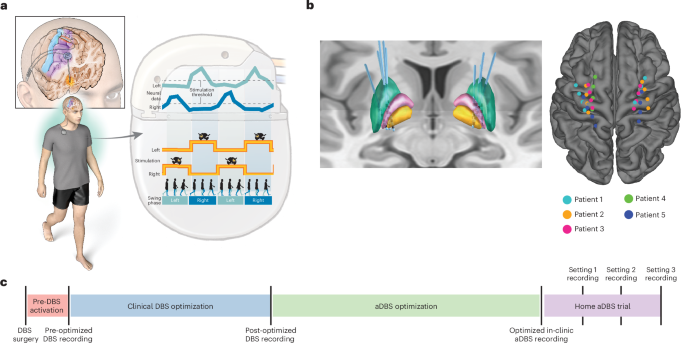
Adaptive DBS (aDBS) represents a shift from “always-on” stimulation to a closed-loop system that adjusts in real-time based on the patient’s brain activity. A 2024 feasibility trial published in Nature Medicine demonstrated that aDBS can track neural biomarkers—specifically beta oscillatory power—to deliver stimulation only when needed. By modulating electrical output based on the brain’s internal state, clinicians can reduce the side effects often associated with constant, high-frequency stimulation, such as speech impairment or dyskinesia, while maintaining control over motor fluctuations.
Can Changing Stimulation Frequency Improve Freezing of Gait?
Yes, adjusting the frequency of stimulation can have significant, albeit sometimes transient, effects on freezing of gait. Clinical evidence published in Movement Disorders and the Journal of Neurology, Neurosurgery & Psychiatry indicates that low-frequency stimulation (typically around 60 Hz to 80 Hz) may offer benefits for patients struggling with FOG that is unresponsive to standard high-frequency settings. While these effects can be immediate, researchers note that the long-term sustainability of low-frequency stimulation often depends on individual factors, including the severity of baseline tremors and the total duration of the patient’s Parkinsonian symptoms.
What Role Do Neural Biomarkers Play in Treatment?
Modern neurostimulation relies on identifying specific “spectral signatures” within the brain. Data from the Brain journal highlights that beta-band oscillations (13–30 Hz) are strongly correlated with akinesia and rigidity. Conversely, gamma oscillations have been linked to dyskinesia. By recording these local field potentials (LFPs), physicians can now “tune” stimulation to suppress pathological beta activity while avoiding the induction of gamma-related side effects. This personalized approach allows for a more nuanced management of motor symptoms that were previously difficult to address with fixed, non-sensing devices.
Summary of Clinical Approaches to DBS
| Method | Mechanism | Primary Target |
|---|---|---|
| Conventional DBS | Continuous, fixed-frequency stimulation | Bradykinesia, tremor |
| Low-Frequency DBS | Reduced frequency (60–80 Hz) | Freezing of gait (FOG) |
| Adaptive DBS (aDBS) | Closed-loop, biomarker-responsive | Fluctuating motor symptoms |
Future Directions in Neuromodulation
The field is moving toward chronic, home-based monitoring where neural data is streamed to clinicians to optimize settings remotely. As noted in Nature Biotechnology, the ability to record brain signals over long periods provides a clearer picture of how Parkinson’s disease evolves after implantation. Future therapies aim to integrate these sensing capabilities with machine learning algorithms to predict gait failure before it happens, potentially offering a proactive rather than reactive approach to managing the disease’s most debilitating motor complications.
