{kind=link}
Disseminated Tuberculosis With Tricuspid Valve Endocarditis: A Diagnostic and Therapeutic Challenge
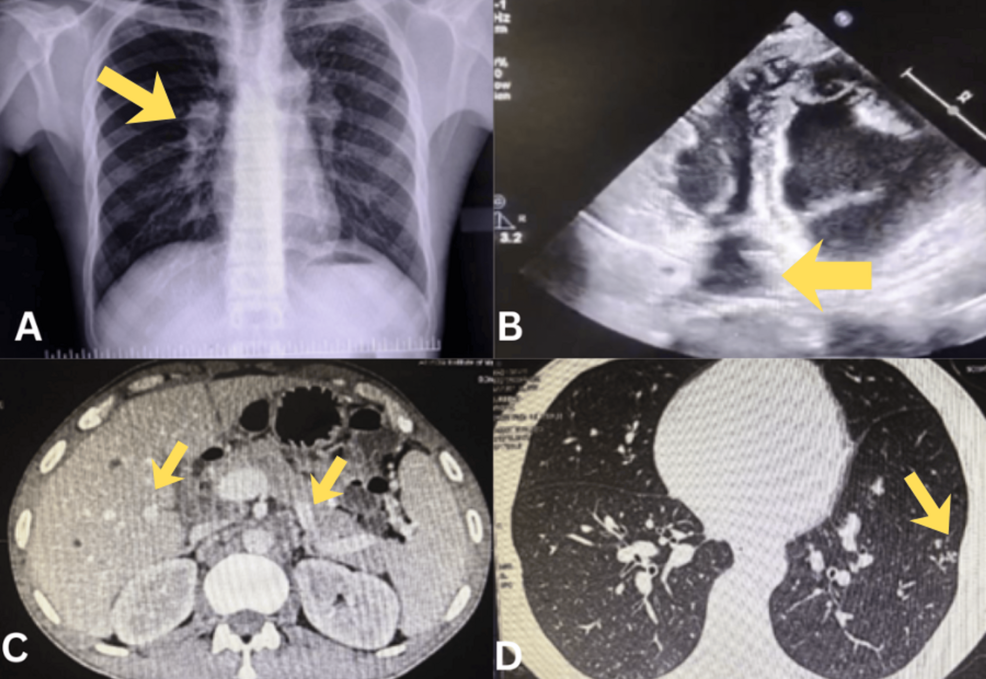
Disseminated tuberculosis (TB), a severe form of the disease where the infection spreads beyond the lungs, can present with rare and complex complications, including endocarditis. One such rare manifestation is tricuspid valve endocarditis, which can mimic culture-negative infective endocarditis, creating significant diagnostic and therapeutic challenges. Understanding this condition requires a nuanced approach, combining clinical expertise, advanced diagnostics, and evidence-based treatment strategies.
Understanding Disseminated Tuberculosis and Endocarditis
Tuberculosis, caused by *Mycobacterium tuberculosis*, typically affects the lungs but can disseminate through the bloodstream, leading to extrapulmonary TB. Disseminated TB is more common in immunocompromised individuals, such as those with HIV, diabetes, or on immunosuppressive therapies. When the infection reaches the heart, it can cause endocarditis—a inflammation of the inner heart lining, often involving the heart valves.
Tricuspid valve endocarditis specifically affects the valve between the right atrium and right ventricle. While bacterial endocarditis is more common, TB can also cause this condition, albeit rarely. The challenge arises because TB-related endocarditis may not be detected through standard culture methods, leading to delayed or missed diagnoses.
Diagnostic Challenges of Culture-Negative Infective Endocarditis
Culture-negative infective endocarditis (IE) occurs when standard microbiological tests fail to identify the causative organism. In TB cases, this can happen due to low bacterial load, prior antibiotic use, or the slow-growing nature of *M. Tuberculosis*. The clinical presentation—fever, fatigue, heart murmurs, and systemic symptoms—overlaps with other forms of IE, complicating differentiation.
Key diagnostic tools include:
- Imaging: Echocardiography (transthoracic or transesophageal) is critical for visualizing valve involvement and detecting vegetations.
- Molecular testing: Polymerase chain reaction (PCR) can identify *M. Tuberculosis* DNA in blood or tissue samples.
- Blood cultures: Despite being negative in some cases, they remain a standard initial step.
- Biopsy: Tissue samples from the affected valve may be necessary for histopathological and microbiological analysis.
The 2015 European Society of Cardiology (ESC) guidelines emphasize the importance of integrating clinical, imaging, and microbiological findings to diagnose IE, including TB-related cases.
Therapeutic Approaches and Management
Treatment of TB-related endocarditis involves a multidisciplinary approach. The standard regimen for TB includes a combination of antibiotics such as isoniazid, rifampin, ethambutol, and pyrazinamide, typically administered for 6–12 months. However, endocarditis may require prolonged therapy, often up to 12 months, to prevent recurrence.
Surgical intervention may be necessary in severe cases, such as when there is significant valve damage, heart failure, or persistent infection despite medical treatment. The UpToDate guidelines highlight the role of surgery in improving outcomes for patients with complicated IE.
Close monitoring for complications, such as embolic events or heart failure, is essential. Patients should also be screened for underlying immunocompromising conditions, as these can influence treatment duration, and response.
Key Takeaways
- Disseminated TB can rarely cause tricuspid valve endocarditis, presenting as culture-negative IE.
- Diagnosis requires a combination of imaging, molecular testing, and clinical evaluation.
- Treatment involves long-term anti-TB therapy, with surgery considered for severe cases.
- Early recognition and multidisciplinary care are critical to improving outcomes.
Future Directions and Research
Research into more rapid and accurate diagnostic tools, such as next-generation sequencing and improved biomarkers, could enhance the detection of TB-related endocarditis. Studies on optimal treatment durations and surgical indications are needed to refine clinical guidelines.

As global TB rates persist, clinicians must remain vigilant about atypical presentations. By integrating emerging evidence with established practices, healthcare providers can better navigate the complexities of this rare but serious condition.
Keep reading