{kind=link}
Frailty as a Predictor of Outcomes in Lower Limb Revascularization and Amputation
Frailty—a clinical syndrome characterized by decreased physiological reserve and increased vulnerability to stressors—serves as a robust predictor of mortality and complications in patients undergoing lower limb revascularization or primary major lower limb amputation. According to research published in Cureus, patients identified as frail face significantly higher rates of postoperative morbidity and long-term mortality compared to non-frail cohorts, regardless of the specific surgical intervention performed.
Why Is Frailty a Critical Surgical Risk Factor?
Frailty represents a systemic decline in biological function, often measured through tools like the Modified Frailty Index (mFI). In the context of vascular surgery, this decline limits a patient’s ability to recover from the intense metabolic demand of major procedures. As noted in the Journal of Vascular Surgery, the presence of frailty is often a more accurate predictor of patient survival than age alone. Because patients requiring revascularization or amputation often present with significant comorbidities—such as diabetes, hypertension, and chronic kidney disease—frailty acts as a multiplier of these baseline risks.
How Does Frailty Affect Amputation Outcomes?
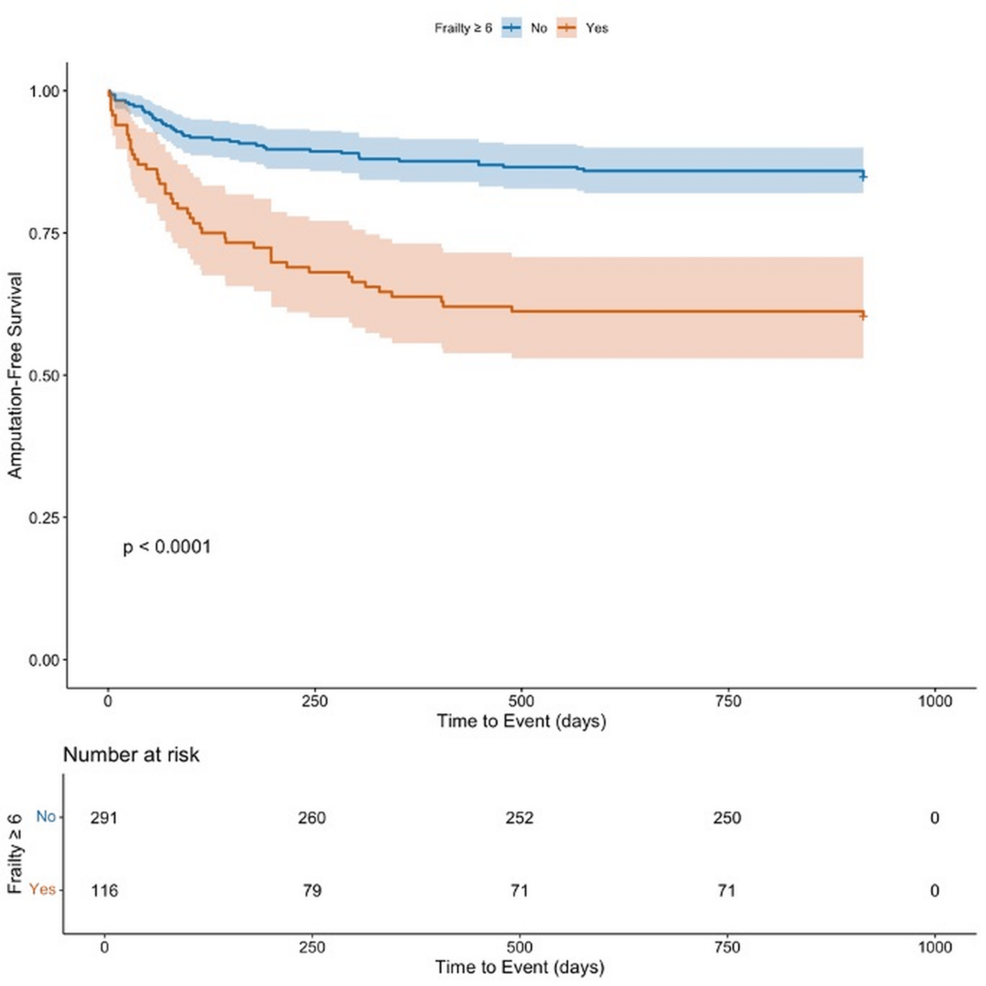
Primary major lower limb amputation is a high-stakes procedure frequently necessitated by advanced peripheral artery disease (PAD) or critical limb ischemia. Research indicates that frail patients undergoing these procedures experience longer hospital stays and a higher probability of discharge to skilled nursing facilities rather than home. Data from the American College of Surgeons suggests that frailty scores correlate linearly with 30-day mortality rates. When surgeons assess a patient, identifying frailty allows for more accurate preoperative counseling, helping families understand the likelihood of functional decline after surgery.
Comparison: Revascularization vs. Amputation
The impact of frailty differs slightly between revascularization (intended to salvage the limb) and amputation (the removal of the limb). The following table summarizes the clinical considerations for both pathways:
| Feature | Revascularization | Amputation |
|---|---|---|
| Primary Goal | Limb salvage and perfusion | Source control of infection/necrosis |
| Frailty Impact | Higher risk of graft failure | Higher risk of poor wound healing |
| Post-Op Recovery | Dependent on vascular patency | Dependent on rehabilitation potential |
What Happens Next for Patient Management?
Clinical teams are increasingly integrating frailty screening into the standard preoperative workup for vascular patients. According to guidelines from the Society for Vascular Surgery, identifying a patient as “frail” does not automatically preclude surgery, but it does shift the focus toward optimization. This may include nutritional support, physical therapy (prehabilitation), and careful management of polypharmacy before the patient enters the operating room. By quantifying frailty, clinicians can better align surgical interventions with the patient’s actual physiological capacity, potentially improving outcomes for those at the highest risk.
Key Takeaways
- Predictive Power: Frailty is an independent risk factor for poor surgical outcomes, often exceeding the predictive value of age or specific comorbidities.
- Clinical Utility: Standardized tools like the Modified Frailty Index (mFI) help surgeons quantify risk and guide shared decision-making.
- Recovery Expectations: Frail patients frequently require extended rehabilitation and have a higher likelihood of non-home discharge following lower limb procedures.
- Preoperative Focus: Prehabilitation efforts directed at nutrition and physical function may mitigate some risks associated with frailty in the vascular surgery population.