{kind=link}
New clinical data indicates that the duration of immunotherapy treatment does not significantly impact disease-free survival (DFS) in patients with mismatch repair-deficient (dMMR) colon cancer. According to findings presented at the European Society for Medical Oncology (ESMO) Congress, short-course neoadjuvant immunotherapy regimens achieve clinical outcomes comparable to longer courses, potentially sparing patients from unnecessary treatment exposure.
Impact of Treatment Duration on DFS
Recent research focused on the neoadjuvant setting—treatment administered before primary surgery—for patients with dMMR, stage III colon cancer. Clinical evidence suggests that the immune system’s response in dMMR tumors is highly sensitive to checkpoint inhibitors.

Data presented regarding these regimens show that patients who received a shorter duration of immunotherapy experienced similar rates of disease-free survival compared to those who underwent longer treatment cycles. This finding is significant because it suggests that the "curative" potential of these drugs is realized early in the treatment course. By limiting the duration, clinicians may reduce the risk of immune-related adverse events without compromising the oncological efficacy of the intervention.
Why dMMR Status Matters in Colon Cancer
Mismatch repair deficiency (dMMR) is a genetic condition where cells fail to repair errors that occur during DNA replication. In the context of colon cancer, dMMR tumors are characterized by a high tumor mutational burden, which makes them particularly recognizable to the immune system.

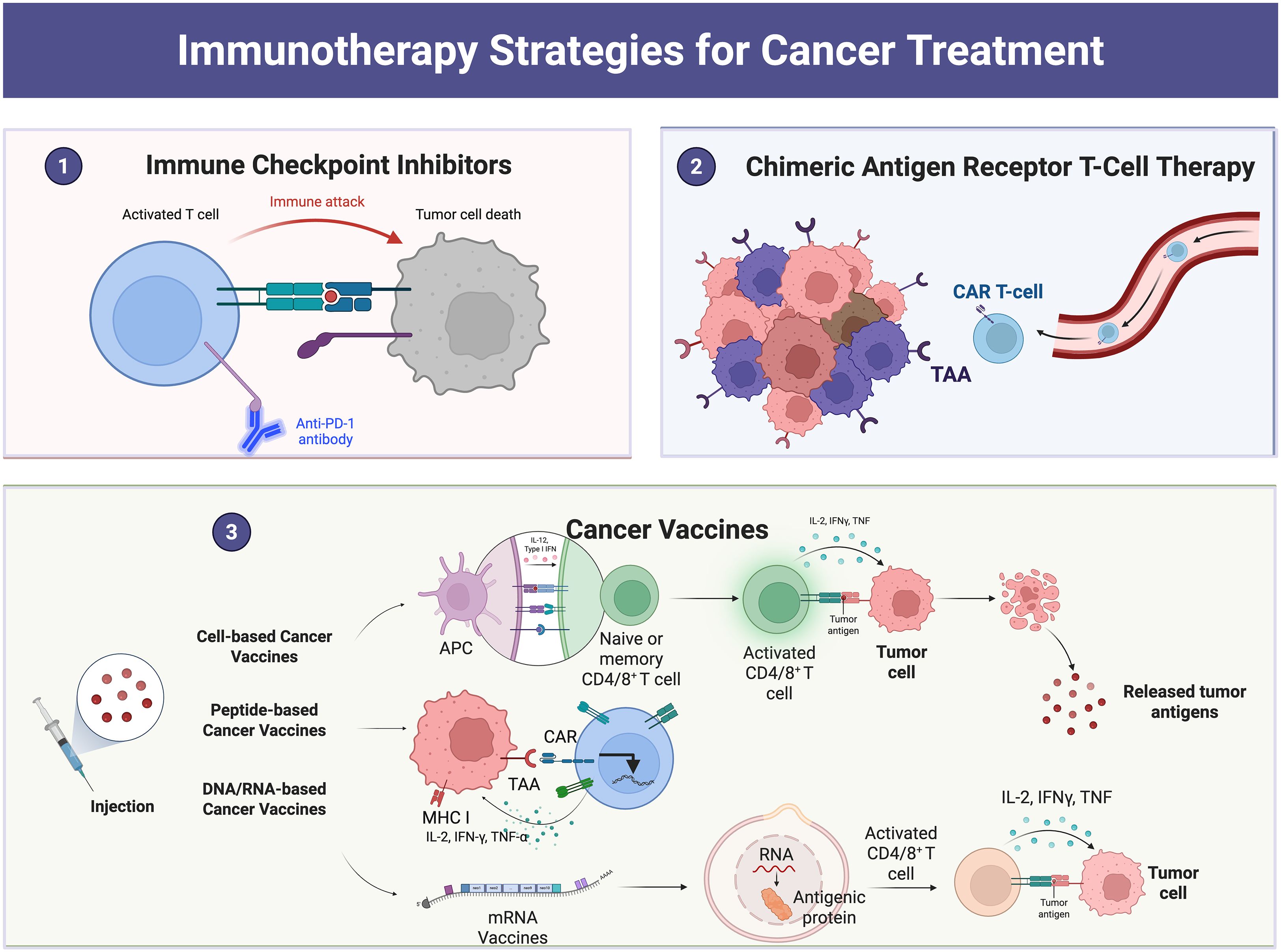
Immunotherapy drugs, such as PD-1 inhibitors, function by "taking the brakes off" the immune system, allowing T-cells to identify and destroy cancer cells more effectively. Because dMMR tumors present more "neoantigens"—abnormal proteins on the cell surface—they are prime targets for this therapeutic approach. The shift toward using these agents in the neoadjuvant setting for stage III disease represents a major change in standard care protocols, moving away from a reliance solely on traditional chemotherapy.
Clinical Implications for Patient Care
The move toward shorter immunotherapy courses aligns with a broader trend in oncology: de-escalation. By identifying the minimum effective dose and duration, medical teams aim to:
- Minimize Toxicity: Reducing exposure lowers the incidence of autoimmune-like side effects, such as colitis, thyroid dysfunction, or dermatitis.
- Improve Quality of Life: Patients spend less time in clinical settings and experience fewer treatment-related complications.
- Optimize Resource Use: Shorter treatment windows can reduce the financial burden on healthcare systems and individual patients.
Comparing Traditional and Modern Approaches
Historically, stage III colon cancer was treated primarily with surgery followed by adjuvant chemotherapy. The integration of immunotherapy changes this sequence.
| Feature | Traditional Chemotherapy | Neoadjuvant Immunotherapy |
|---|---|---|
| Primary Mechanism | Cytotoxic DNA damage | Immune system activation |
| Timing | Post-surgery (Adjuvant) | Pre-surgery (Neoadjuvant) |
| Duration | Fixed (often 3–6 months) | Variable (now being optimized) |
| Target | Rapidly dividing cells | PD-1/PD-L1 pathways |
The current data suggests that for the dMMR subpopulation, the "more is better" philosophy of traditional chemotherapy does not necessarily apply to immunotherapy. As clinical trials continue to mature, oncologists are expected to refine these protocols further to ensure that treatment duration is tailored to individual patient response rather than a one-size-fits-all duration.