{kind=link}
Medicaid State Directed Payments Face $911 Billion Federal Spending Reduction
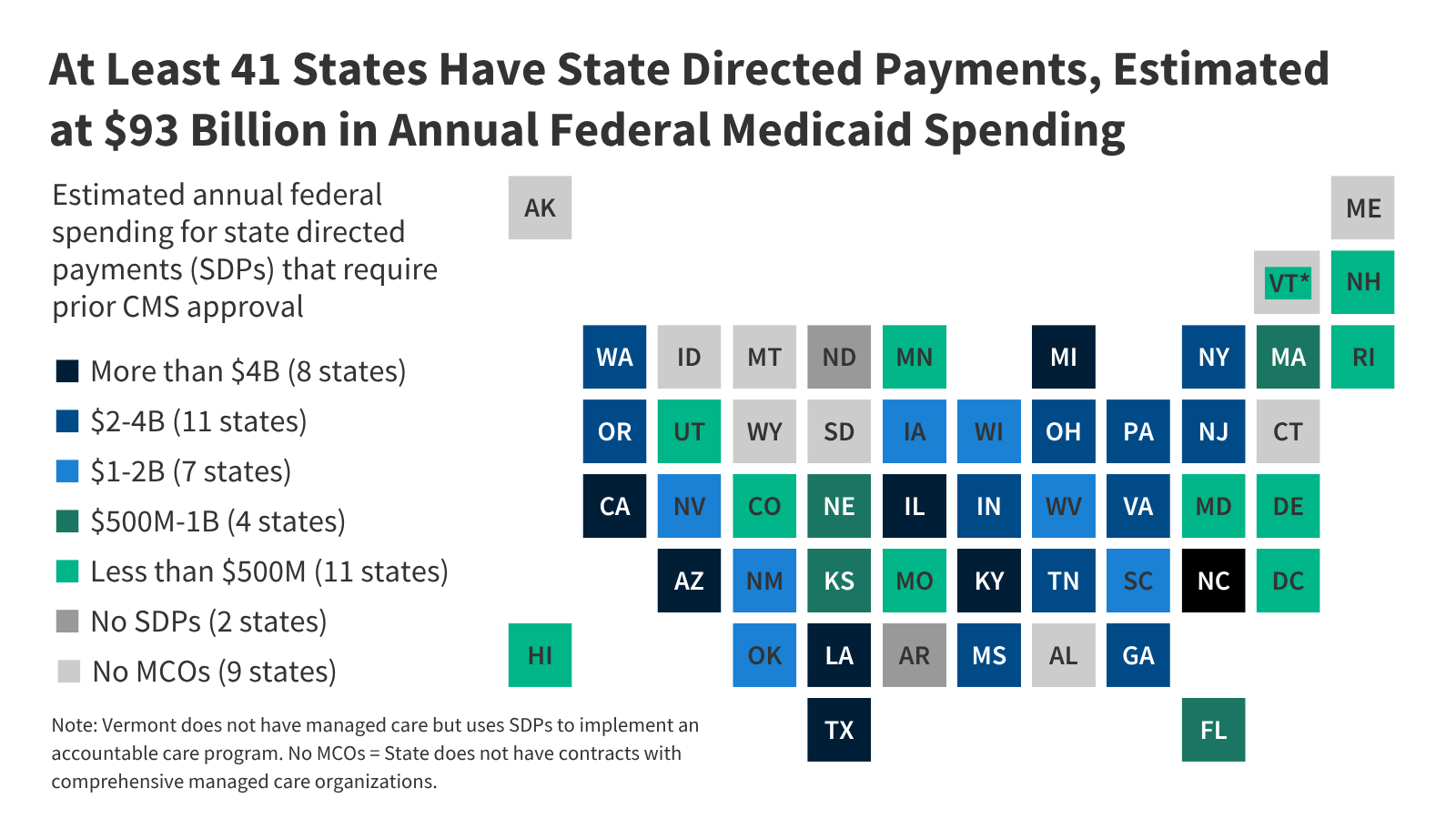
New federal legislation will reduce Medicaid spending by an estimated $911 billion between 2025 and 2034, largely by placing stricter limits on state directed payments (SDPs) for hospital and clinical services. These payments, which allow states to mandate that managed care organizations (MCOs) pay specific rates to providers, have become a primary, though inconsistently regulated, vehicle for supplemental Medicaid funding. According to data analyzed by KFF, total annual spending through these mechanisms currently reaches approximately $137 billion, with the federal government covering $93 billion of that total.
How State Directed Payments Currently Function
State directed payments act as a bridge between state Medicaid agencies and the private managed care plans that oversee the majority of Medicaid enrollees. While states are typically prohibited from dictating how MCOs handle provider contracts, the Centers for Medicare and Medicaid Services (CMS) allows SDPs to ensure specific minimum payment rates or uniform rate increases for services.
States use these payments to bolster provider participation and improve access to care. However, the financing of these programs is often complex. Many states rely on intergovernmental transfers—often from public hospitals—or provider taxes to fund the state share of these payments. Research from the CMS proposed rule on SDPs indicates that 81% of SDPs with payment rates exceeding Medicare levels are financed, in whole or in part, by these provider-linked revenue sources.
Which Services Receive the Most Funding?

The vast majority of federal spending through SDPs is concentrated in the hospital sector. Approximately 84% of the $93 billion in annual federal SDP spending is directed toward hospital services, according to KFF’s analysis of 305 approved preprints.
Beyond general hospital services, smaller portions of funding are allocated to:
- Professional services at academic medical centers
- Nursing facility services
- Behavioral health services
The reliance on these payments is widespread, with 41 states—including the District of Columbia—utilizing SDPs to supplement Medicaid reimbursements. California leads the nation in projected federal SDP spending at $10.6 billion, followed by Texas, North Carolina, and Illinois.
Why Data Gaps Complicate Oversight
A significant challenge in managing SDPs is the lack of standardized, transparent reporting. States submit “preprints” to CMS to gain approval for these programs, but these documents often contain incomplete information regarding specific payment levels or financing structures.
Furthermore, current regulations create an oversight loophole: if a state mandates that MCOs pay exactly the Medicare or Medicaid fee-for-service (FFS) rate, they are not required to submit a preprint to CMS. This means the total volume of Medicaid spending flowing through state-directed arrangements is likely higher than what is captured in official preprint data. To address this, CMS issued guidance in March 2026 requiring states to begin reporting actual paid amounts via the Transformed Medicaid Statistical Information System (T-MSIS) by September 2026.
Impact of the 2025 Reconciliation Law

The 2025 reconciliation law introduces a shift in how these payments will be permitted moving forward. By establishing stricter federal oversight, the law aims to curb the rapid growth of supplemental payments that have functioned as indirect ways to increase provider reimbursement.
While the policy goal is to stabilize long-term federal Medicaid spending, providers and state agencies face potential budget volatility. States with a high reliance on SDPs to maintain hospital solvency may need to restructure their provider payment models to align with the new federal benchmarks. The transition will likely force states to move away from complex, tax-funded supplemental payment schemes toward more transparent, value-based reimbursement structures.
Key Takeaways
- Federal Reduction: The 2025 reconciliation law targets $911 billion in federal savings over a decade, with SDP restrictions as a core component.
- Current Volume: Annual federal spending through SDPs is estimated at $93 billion, with 84% of those funds supporting hospital services.
- Transparency Issues: CMS has mandated new T-MSIS reporting requirements to close data gaps that have historically obscured the true cost and financing of these payments.
- Provider Dependency: Because 81% of higher-rate SDPs rely on provider taxes or intergovernmental transfers, the new limits may significantly impact the net revenue of hospital systems in participating states.
Related reading