{kind=link}
Medicaid programs across the United States are currently navigating a complex legal and regulatory landscape regarding new community engagement requirements. As of mid-2026, federal rules necessitate that states implement work or community engagement mandates for certain Medicaid enrollees, while providing exemptions for those deemed "medically frail." The criteria for these exemptions, specifically the requirement that a condition must significantly impair an individual’s ability to work, have sparked litigation from multiple states challenging the scope of federal oversight.
Federal Requirements for Medicaid Community Engagement
The Centers for Medicare and Medicaid Services (CMS) issued an interim final rule on June 1, 2026, to guide states in implementing community engagement requirements under the 2025 federal budget reconciliation law. This law targets Medicaid enrollees covered through Affordable Care Act (ACA) expansion or specific waivers.

To maintain eligibility, enrollees must either meet work requirements or qualify for an exclusion. The federal rule establishes a two-part test for the "medically frail" exclusion. An individual must not only have a qualifying medical condition but also demonstrate that the condition limits their capacity to fulfill community engagement obligations. This approach represents a shift from earlier state-level expectations, where some states, such as Nebraska, initially moved toward excluding individuals based solely on the presence of a specific diagnosis.
Legal Challenges to the CMS Rule
On June 29, 2026, a coalition of 24 states and two governors filed a lawsuit in the U.S. District Court for the District of Massachusetts. The plaintiffs argue that the CMS requirement—which mandates that a condition must "significantly impair" an individual’s ability to comply—exceeds the authority granted by the reconciliation law.

According to the legal filing, the plaintiff states contend that the law’s statutory exclusions were intended to protect vulnerable populations, including those with disabilities or serious health conditions like cancer. The states argue that forcing these individuals to prove functional impairment to retain coverage creates unnecessary risks to patient health. The court has yet to rule on the request to enjoin or vacate the two-part test.
Impact on Medicaid Coverage for People with HIV
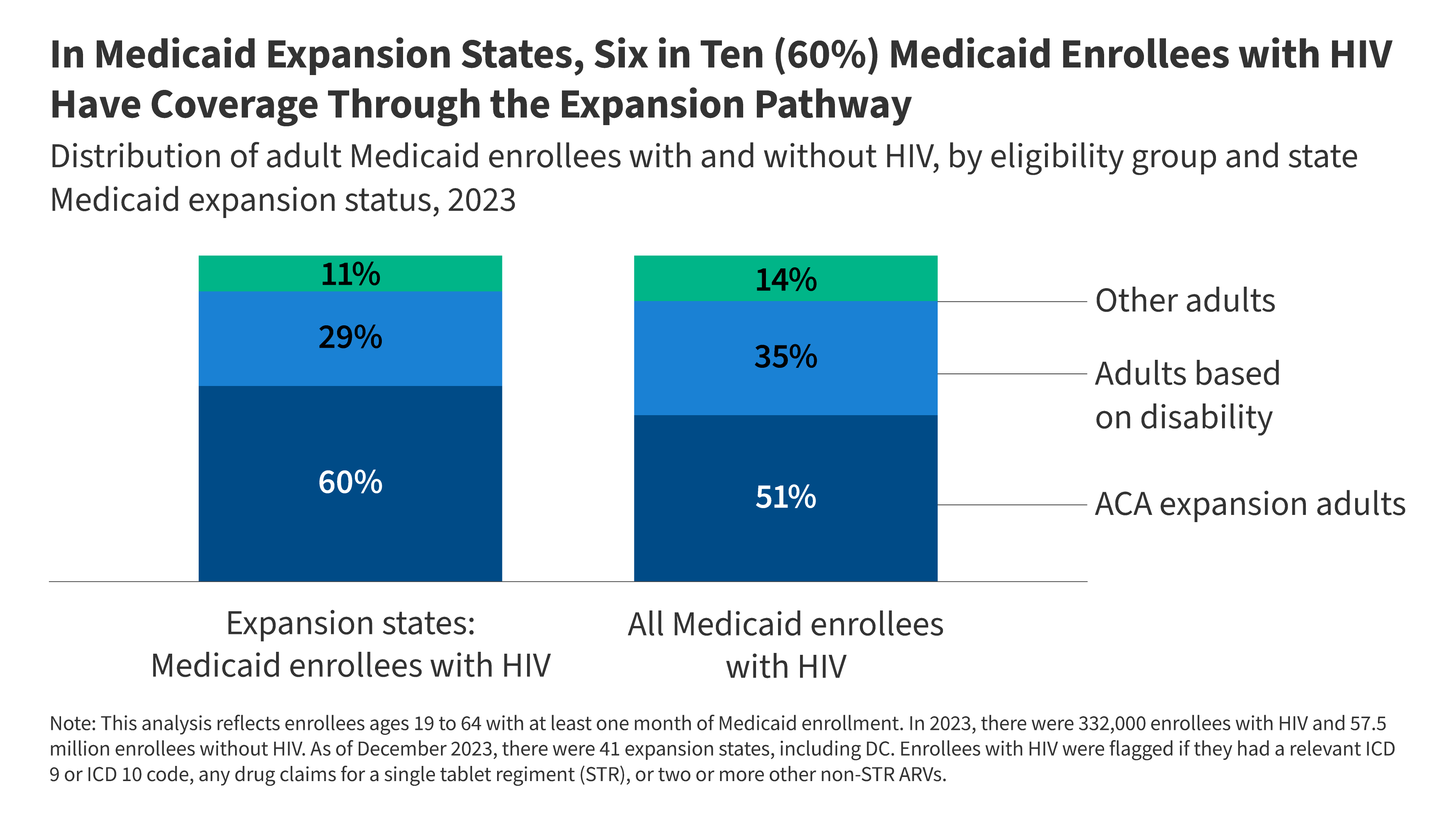
Medicaid serves as a vital source of coverage for people with HIV, with 46% of the population relying on the program as of 2023. In states that expanded Medicaid, the expansion pathway accounts for 60% of coverage for adults under age 65 with HIV.
The new federal rule identifies HIV/AIDS as an example of a "serious or complex" condition. However, it clarifies that a diagnosis alone is insufficient for an exemption; the condition must be shown to impair the ability to work. For those with well-managed HIV, this creates a potential barrier to exemption. While many people with HIV have comorbidities—73% of Medicaid-enrolled individuals with HIV have chronic conditions other than the virus—the administrative burden of documentation could lead to coverage gaps.
Administrative Barriers and Privacy Concerns
The requirement for states to maintain an auditable list of diagnosis codes for medical frailty introduces several operational hurdles:

- Verification Methods: Because the rule rejects the use of diagnoses alone for exemptions, states cannot rely solely on automated, ex parte data processing. They must implement alternative verification methods, such as health screeners or provider documentation.
- Privacy and Data Sharing: Some states are evaluating data-sharing agreements between Medicaid agencies and public health departments to identify enrollees. This process raises concerns regarding the security of sensitive HIV-related health data.
- Provider Burden: While the rule allows clinicians, including clinical social workers, to provide documentation, the requirement to assess a patient’s functional impairment adds significant administrative work to clinics that already manage complex care coordination.
Public Health Implications
The potential for coverage loss poses risks to both individual and public health. Research suggests that treatment interruptions can lead to antiretroviral resistance and increased HIV transmission rates. Furthermore, if individuals lose Medicaid coverage, they may turn to the federal Ryan White Program, which is already facing budget constraints in several states.
As litigation continues, the implementation of these requirements remains in flux. The conflict centers on the balance between federal program oversight and the necessity of ensuring that the most vulnerable patients maintain consistent access to life-saving care.