{kind=link}
Understanding Dieulafoy’s Lesion: A Rare but Critical Cause of Gastrointestinal Bleeding
Gastrointestinal (GI) bleeding can be a frightening experience, often requiring urgent medical evaluation to determine the source. While common causes like peptic ulcers or diverticulosis are frequently discussed, some conditions are significantly rarer and more elusive. One such condition is the Dieulafoy’s lesion, a vascular anomaly that, while uncommon, can cause life-threatening hemorrhage if not identified and treated promptly.
What is a Dieulafoy’s Lesion?
A Dieulafoy’s lesion is a rare type of vascular malformation characterized by a large, tortuous artery that erodes through the gastrointestinal mucosa. Unlike a typical ulcer, which involves the gradual wearing away of the stomach or intestinal lining, a Dieulafoy’s lesion occurs when an abnormally large artery—often referred to as a “pinpoint” vessel—ruptures through the surface layer without an underlying ulcer or tumor.
Because the vessel is unusually large (often 1 to 5 mm in diameter) and sits just beneath the surface, it can lead to sudden, massive, and recurrent bleeding. While these lesions are most commonly found in the stomach, they can occur anywhere along the gastrointestinal tract, including the duodenum, esophagus, and colon.
Why the Duodenum Is a Notable Site
Most Dieulafoy’s lesions are identified in the proximal stomach, specifically along the lesser curvature. However, when these lesions manifest in the second portion of the duodenum—the part of the small intestine where the bile and pancreatic ducts enter—they present unique diagnostic and therapeutic challenges. The proximity to vital structures and the anatomy of the small bowel require high clinical suspicion and specialized endoscopic skills to manage effectively.
Symptoms and Clinical Presentation
The hallmark of a Dieulafoy’s lesion is painless but significant gastrointestinal bleeding. Patients typically present with one or more of the following:
- Hematemesis: Vomiting blood or material that looks like coffee grounds.
- Melena: Passing black, tarry stools, which indicates bleeding in the upper GI tract.
- Hematochezia: Bright red blood in the stool, which can occur if the bleeding is rapid or originating from the lower tract.
- Signs of Anemia: Dizziness, shortness of breath, or pale skin due to blood loss.
Because the bleeding is often intermittent and the surrounding tissue may appear normal during a standard examination, these lesions are frequently missed during initial endoscopies.
Diagnosis and Management
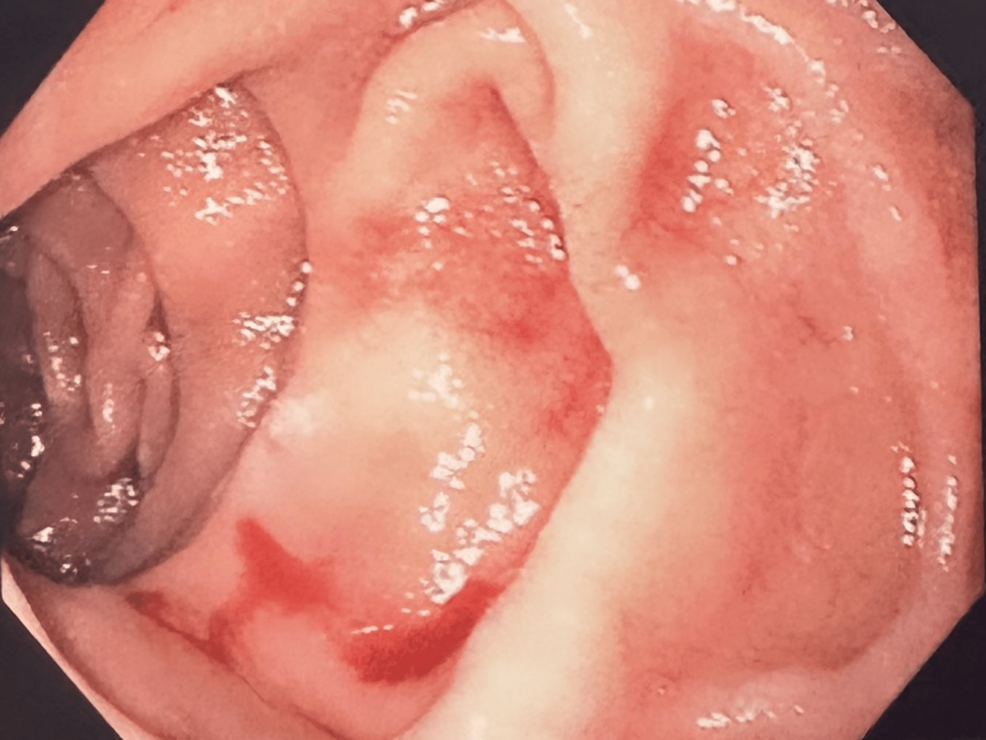
Diagnosis is primarily achieved through an upper endoscopy (EGD). During the procedure, a gastroenterologist looks for a small, isolated vessel protruding through a minute defect in the mucosa, often surrounded by normal-appearing tissue. If the lesion is actively bleeding, it may present as a “spurting” vessel.

Endoscopic Hemostasis: The Gold Standard
Modern medicine has shifted away from surgical intervention for these lesions in favor of minimally invasive endoscopic techniques. Once identified, a Dieulafoy’s lesion can usually be treated during the same procedure using several methods:
- Endoscopic Clipping: Placing a mechanical clip over the vessel to pinch it shut.
- Thermal Therapy: Using heat (like bipolar electrocoagulation) to seal the vessel.
- Injection Therapy: Injecting epinephrine around the lesion to constrict the blood vessel and stop the flow.
These techniques are highly effective, with success rates reported in the literature as being excellent for preventing re-bleeding.
Key Takeaways
- High Suspicion: Dieulafoy’s lesion should be considered in patients with unexplained upper GI bleeding, even if initial tests are negative.
- Vascular Origin: It is not an ulcer; it is a structural abnormality of a blood vessel that erodes through the intestinal lining.
- Effective Treatment: Endoscopic intervention is the first-line treatment and is typically successful, avoiding the need for invasive surgery.
- Prompt Evaluation: Because bleeding can be massive, urgent medical assessment in an emergency setting is vital.
Frequently Asked Questions (FAQ)
Is a Dieulafoy’s lesion cancerous?
No, a Dieulafoy’s lesion is a benign vascular anomaly. It is not a tumor and does not have the potential to become cancerous.
Can these lesions heal on their own?
While the bleeding may stop temporarily, the underlying exposed artery remains, meaning the risk of recurrent, potentially life-threatening hemorrhage is very high. Medical intervention is always required.
What should I do if I see blood in my stool?
Any instance of blood in the stool or vomiting of blood requires immediate medical attention. Seek emergency care to stabilize your condition and allow for a professional evaluation of the source of the bleeding.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.