{kind=link}
In Vivo CAR-T Cell Therapy Shows Promise for Multiple Myeloma
A new approach to CAR-T cell therapy, involving the generation of these immune cells directly within the patient’s body, is demonstrating encouraging early results in the treatment of relapsed or refractory multiple myeloma. This innovative technique bypasses the traditional, more complex process of ex vivo manufacturing and lymphodepletion, potentially offering a faster and more accessible path to this powerful immunotherapy.
Understanding CAR-T Cell Therapy
Chimeric antigen receptor (CAR) T-cell therapy is a type of immunotherapy that harnesses the patient’s own immune system to fight cancer. T cells, a type of white blood cell, are engineered to express a CAR that recognizes a specific protein on cancer cells. These modified T cells are then infused back into the patient, where they can target and destroy cancer cells. Traditionally, this process involves removing T cells from the patient (ex vivo), genetically modifying them in a lab and then infusing them back into the patient after lymphodepleting chemotherapy.
The In Vivo Approach: A Simplified Process
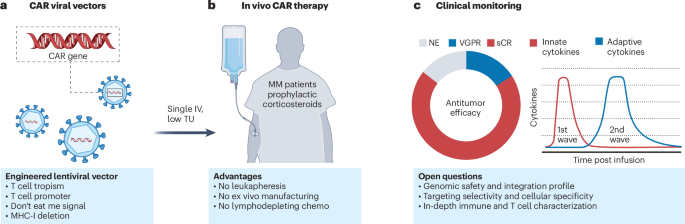
The in vivo approach, as detailed in recent research published in Nature Medicine, utilizes a nanobody-directed, immune-shielded lentiviral vector encoding a humanized anti-B cell maturation antigen (BCMA) CAR. This vector is administered directly to the patient via intravenous infusion, prompting the generation of CAR-T cells within the body itself. This eliminates the need for leukapheresis, ex vivo manufacturing, and lymphodepleting chemotherapy – streamlining the process considerably.
Early Clinical Trial Results
A phase 1, single-arm, open-label trial involving five heavily pretreated patients with relapsed or refractory multiple myeloma evaluated the safety and tolerability of ESO-T01, the in vivo CAR-T cell therapy. The trial, which was stopped early in 2025 after initial enrollment, showed no dose-limiting toxicities. However, all patients experienced grade 3 or higher adverse events.
- Cytokine Release Syndrome (CRS): Four patients developed CRS, with three cases classified as grade 3 and one as grade 2. CRS was managed with corticosteroids, tocilizumab, or supportive care.
- Cytopenias & Liver Enzyme Elevations: Transient cytopenias and reversible hepatic enzyme elevations were common toxicities.
- Infections: Three patients experienced grade 2 infections.
- Neurotoxicity & Mortality: One patient experienced grade 1 immune effector cell-associated neurotoxicity and unfortunately died from extramedullary lesion-related spinal cord compression.
Antimyeloma Activity Observed
Despite the adverse events, preliminary data indicated promising antimyeloma activity. Four of the five patients achieved objective responses, including three stringent complete remissions. Minimal residual disease negativity (10-5) was observed in all evaluable responders (4/4) by day 60. Further research suggests this approach offers key mechanistic insights into CAR-T cell therapy.
The Future of CAR-T Cell Therapy
The development of in vivo CAR-T cell therapy represents a significant step forward in the field of immunotherapy for multiple myeloma. As highlighted in a recent review, ongoing research focuses on improving CAR-T cell efficacy by addressing challenges such as BCMA loss, the immunosuppressive tumor microenvironment, and safety concerns like cytokine release syndrome and neurotoxicity. This innovative approach has the potential to make CAR-T cell therapy more accessible and efficient, offering new hope for patients with this challenging cancer.
Key Takeaways
- In vivo CAR-T cell generation bypasses ex vivo manufacturing and lymphodepletion.
- Early clinical trials show promising antimyeloma activity, with objective responses observed in a majority of patients.
- The therapy is associated with adverse events, including cytokine release syndrome and neurotoxicity, requiring careful management.
- Ongoing research aims to optimize the efficacy and safety of in vivo CAR-T cell therapy.
Keep reading