{kind=link}
Why Viral Load Doesn’t Predict Symptoms in Influenza A(H3N2) Infections
Recent clinical research published in Nature Medicine demonstrates that the severity of influenza A(H3N2) symptoms is not determined by the amount of virus present in the body, but rather by the speed and intensity of the host’s early innate immune response. While symptomatic and asymptomatic individuals show similar viral loads during the acute phase of infection, those who experience symptoms exhibit an earlier and more robust activation of systemic myeloid cells and inflammatory mediators.
Why do some people remain asymptomatic?
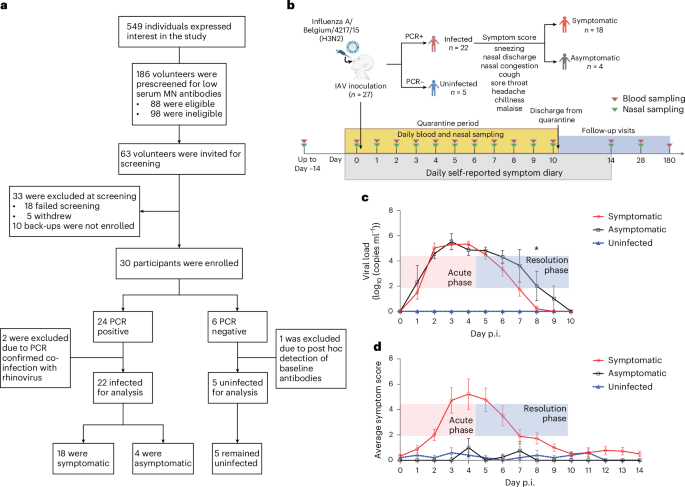
Asymptomatic infection in influenza is not merely a result of lower viral replication. According to the study involving 27 healthy adult volunteers, individuals who remained asymptomatic showed no significant difference in peak viral load compared to those who developed symptoms. Instead, the distinction lies in the immune system’s “trigger” threshold. Symptomatic participants demonstrated a rapid, intense induction of pro-inflammatory cytokines—including IFNγ, IL-6, and TNF—within the first two to three days post-inoculation. In contrast, asymptomatic participants maintained a more tempered immune profile, avoiding the systemic inflammatory cascade that drives clinical illness.
How does the immune system drive symptoms?
Symptoms are largely a byproduct of an exaggerated early innate response rather than the virus itself. The research highlights a clear temporal link: early activation of circulating monocytes and dendritic cells, marked by the expression of CD169 and HLA-ABC, correlates strongly with higher symptom scores. This early myeloid activation serves as a precursor to a secondary wave of adaptive immune activity. By day seven, symptomatic individuals showed a significantly higher proliferation of natural killer (NK) cells and CD8+ T cells compared to asymptomatic counterparts. This suggests that while an aggressive immune response clears the virus more rapidly, it simultaneously produces the systemic inflammation felt by the patient as fever, malaise, and respiratory distress.
What role does pre-infection immunity play?
A person’s susceptibility to symptomatic disease appears to be linked to their baseline immune responsiveness. When researchers stimulated pre-inoculation blood samples from volunteers with heat-inactivated influenza virus, those who later developed symptomatic infections showed a significantly higher secretion of IL-1β. This suggests that certain individuals possess “hyper-responsive” myeloid cells that react more aggressively upon initial viral exposure. This heightened sensitivity is not permanent; the study found that after the initial infection, immune cells entered a temporary state of “refractoriness,” showing reduced cytokine production when challenged with the virus again, before eventually returning to baseline levels by day 28.
Key Takeaways
- Viral Load Disconnect: Peak viral load does not predict whether an influenza infection will be symptomatic.
- Inflammatory Drivers: Symptoms are driven by an early, exaggerated systemic innate immune response, particularly involving monocytes and dendritic cells.
- Predictive Markers: High expression of CD169 and HLA-ABC on circulating immune cells in the first 72 hours is a reliable indicator of subsequent symptom severity.
- Baseline Sensitivity: Individuals with higher baseline IL-1β production in response to viral stimulation are more likely to experience symptomatic illness.
What happens next for influenza research?
These findings shift the focus of influenza treatment from purely antiviral strategies toward immune-modulating approaches. By identifying the specific temporal “bottlenecks”—such as the IL-15 mediated feedback loop that activates NK cells—researchers may eventually develop therapies that balance viral clearance with the prevention of excessive inflammation. Future studies will need to determine if these innate immune signatures hold true across different influenza strains and in more diverse, older, or immunocompromised populations, as this study was limited to healthy adults aged 18 to 55.