{kind=link}
Medicaid Faces Pressure as Prescription Drug Costs Rise
Medicaid, the primary health coverage program for low-income individuals, is grappling with increasing prescription drug expenditures, particularly for new, high-cost medications like GLP-1s and cell and gene therapies. This challenge occurs alongside a tightening fiscal environment and federal funding adjustments, placing pressure on state Medicaid programs to manage costs effectively. Recent initiatives from the Trump administration aim to address these rising costs, but their impact remains uncertain.
Drug Spending Within the Broader Medicaid Budget
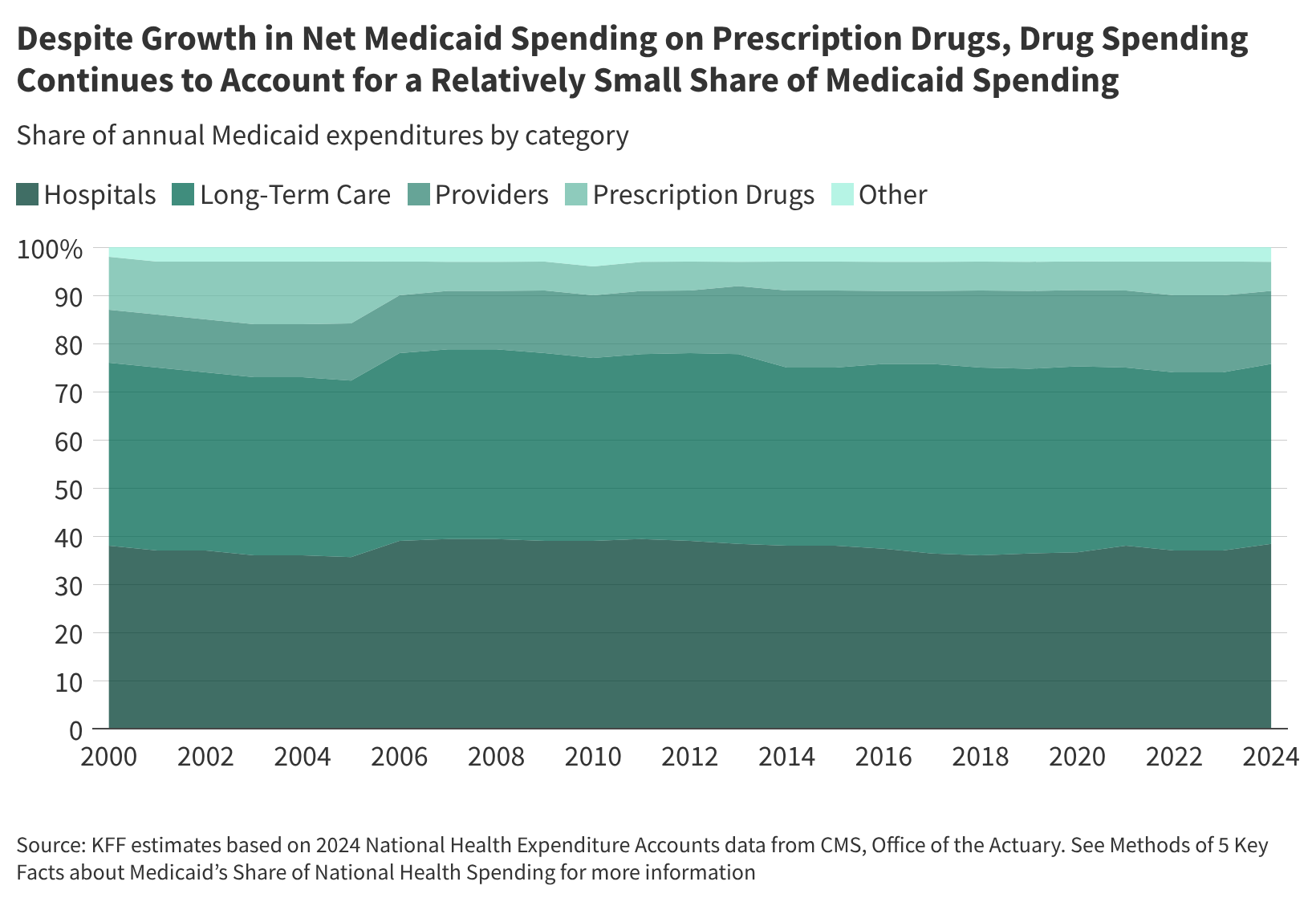
While Medicaid spending on prescription drugs has grown, it still represents a relatively little portion of overall Medicaid expenditures. In 2024, drug spending accounted for 6% of the total Medicaid budget, compared to 38% for hospital care, 37% for long-term care, and 15% for provider services [1]. This percentage has remained relatively stable—between 5% and 7%—since the implementation of the Medicare prescription drug benefit in 2006. Although, net spending on prescription drugs increased by 46% between federal fiscal year 2019 and 2024, mirroring the overall growth in Medicaid spending (52%) [1]. States have reported increasing pharmacy costs as a significant budget pressure [1].
Affordability for Enrollees
Federal law limits out-of-pocket costs for Medicaid enrollees, ensuring access to needed prescriptions with minimal financial burden. Copays are capped at $4 for preferred drugs and $8 for non-preferred drugs for those with incomes at or below 150% of the federal poverty level (FPL), with slightly higher amounts for those with higher incomes [1]. Many populations, such as children under 18 and pregnant women, are exempt from cost-sharing requirements. Over two-thirds of Medicaid enrollees take prescription medications, a rate similar to those with private insurance (68%), but significantly higher than uninsured adults (37%) [1]. Uninsured adults are more likely to delay or forgo needed prescriptions due to cost (17%) compared to Medicaid (10%) and privately insured adults (8%) [1].
State Administration of the Pharmacy Benefit
All state Medicaid programs cover prescription drugs, but they administer the benefit in various ways. As of July 2025, eight out of 42 states contracting with managed care organizations (MCOs) carve out prescription drug coverage from managed care, delivering the pharmacy benefit through fee-for-service (FFS) [1]. Most states utilize capitated managed care, and many contract with pharmacy benefit managers (PBMs) to manage or administer the pharmacy benefit, whether in FFS or managed care settings. As of July 1, 2023, 33 states reported contracting with a PBM for their FFS pharmacy benefit [1]. PBMs are facing increased scrutiny, leading to state-level reforms aimed at increasing transparency, and oversight.
Medicaid Drug Payment Policies
Total Medicaid spending for a drug is determined by the payment to the pharmacy less any rebates received from the manufacturer. Payments are based on the ingredient cost of the drug and professional dispensing fees, plus enrollee copays [1]. Federal regulations guide FFS payment levels, while MCOs have more flexibility. The final cost is offset by rebates from the Medicaid Drug Rebate Program (MDRP) and any state-negotiated supplemental rebates. Under the MDRP, manufacturers must rebate a portion of drug payments in exchange for Medicaid coverage of their products [1].
Strategies for Cost Management
States employ various strategies to manage prescription drug expenditures, including prior authorization, preferred drug lists (PDLs), step therapy, and quantity limits [1]. Many states negotiate supplemental rebates with manufacturers, and some participate in multi-state purchasing pools or value-based arrangements. The Centers for Medicare & Medicaid Services (CMS) has also launched new payment models aimed at combating rising costs, though the impact of these models is still being evaluated [2], [3].
The BALANCE Model
CMS recently announced the Better Approaches to Lifestyle and Nutrition for Comprehensive hEalth (BALANCE) Model, a voluntary test designed to enable Medicare Part D plans and state Medicaid agencies to cover GLP-1 medications for weight management and metabolic health improvement while controlling costs [3]. This model involves negotiating directly with pharmaceutical manufacturers for lower net prices, standardized coverage terms, and evidence-based lifestyle support offerings [3].
Worth a look