{kind=link}
Precision Immunotherapy Shows Promise in Pancreatic Cancer with Genetic Insights
A new study published in Nature highlights encouraging results from the POLAR trial, investigating a precision immunotherapy approach for metastatic pancreatic cancer (mPC). The trial focuses on tailoring treatment based on a patient’s genetic profile, specifically homologous recombination deficiency (HRD), and its impact on response to a combination of pembrolizumab and olaparib.
Understanding Homologous Recombination Deficiency (HRD)
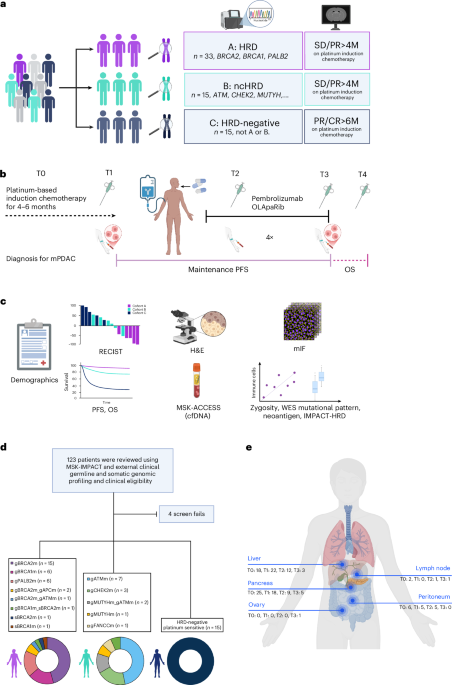
HRD refers to defects in genes responsible for repairing DNA damage. Mutations in genes like BRCA1, BRCA2, and PALB2 are key indicators of HRD. The POLAR trial categorized patients into three cohorts based on their HRD status and response to platinum-based chemotherapy:
- Cohort A (HRD): Patients with mutations in core HRR genes (BRCA2, BRCA1, and PALB2) who did not experience disease progression for over 4 months during platinum-based chemotherapy.
- Cohort B (ncHRD): Patients with mutations in non-core HRR genes (ATM, BAP1, BARD1, BLM, BRIP1, CHEK2, FAM175A, Fance, FANCC, NBN, RAD50, RAD51, RTEL1 and MUTYH) also without disease progression for over 4 months.
- Cohort C (HRD Negative): Patients who remained stable on platinum-based chemotherapy for at least 6 months but lacked HRD or ncHRD gene mutations.
Trial Design and Key Findings
The POLAR trial enrolled 63 participants between January 2021 and March 2024. All participants received a maintenance regimen of olaparib and pembrolizumab. Researchers collected serial tumor tissue and blood samples to analyze genomic instability, the tumor immune microenvironment, and neoantigen landscapes.
While the trial did not meet its primary endpoint of a 6-month progression-free survival (PFS) rate of 77% in cohort A, significant findings emerged:
- Objective Response Rate (ORR): ORR was 35% (7/20) in cohort A, 8% (1/12) in cohort B, and 14% (2/14) in cohort C.
- PFS: Median PFS was 8.3 months in cohort A, 4.8 months in cohort B, and 3.3 months in cohort C.
- Overall Survival (OS): Median follow-up was 37 months. The 2-year OS rate was 56% in cohort A.
Biomarker Insights and ctDNA Analysis
Exploratory analyses revealed that patients in cohort A with durable PFS (over 4 months) had a response rate of 52%. Analysis of circulating tumor DNA (ctDNA) showed that changes in variant allele frequency (VAF) between baseline and 6 weeks correlated with PFS. Participants with undetectable or near-undetectable VAF at both timepoints demonstrated durable clinical benefit.
Whole-exome sequencing (WES) showed that cohort A tumors had a more immunogenic mutational landscape, with higher indel burden and frameshift indel burden compared to cohort C. This suggests a greater potential for the immune system to recognize and attack these cancer cells.
Immune Infiltration and Treatment Response
Tumors in cohort A exhibited greater tumor-infiltrating lymphocyte (TIL) density on H&E staining compared to cohort C. Multiplex immunofluorescence (mIF) analysis revealed higher CD3+CD8+ T cell infiltration in cohort A, correlating with longer PFS. Yet, CD8+ T cell infiltration did not correlate with neoantigen burden.
Safety Profile
The treatment combination of olaparib and pembrolizumab was generally well-tolerated. No grade 4 or 5 treatment-related adverse events occurred. The most common grade 3 adverse events included anemia and abdominal infection. Immune-related adverse events were manageable.
Implications for Future Treatment
The POLAR trial demonstrates the potential of biomarker-guided precision immunotherapy in metastatic pancreatic cancer. Identifying patients with HRD mutations and monitoring ctDNA dynamics may help predict treatment response and personalize therapy. Further research is needed to optimize treatment strategies and explore the role of the tumor immune microenvironment in enhancing immunotherapy efficacy. A related phase II trial is evaluating olaparib plus pembrolizumab versus olaparib alone as maintenance therapy for patients with metastatic pancreatic cancer and germline BRCA1 or BRCA2 mutations (SWOG S2001 NCT04548752).
Other research is also exploring combinations of immunotherapies, such as avelumab and talazoparib, in solid tumors with BRCA1/2 or ATM alterations (Avelumab Plus Talazoparib in BRCA1/2 or ATM-Altered Solid Tumors).
Related reading