{kind=link}
Preeclampsia is a life-threatening pregnancy complication that has long lacked a disease-specific treatment. For women facing very preterm preeclampsia, the stakes are incredibly high, often requiring a challenging balance between maternal safety and fetal maturity. However, a groundbreaking first-in-human trial published in Nature Medicine suggests we may be entering a new era of targeted therapy. By selectively removing a specific placental protein from the blood, researchers have demonstrated a safe way to potentially extend pregnancies and manage blood pressure.
Understanding the Culprit: What is sFlt-1?
To understand this breakthrough, we first have to look at the biology of preeclampsia. The placenta secretes a protein called soluble Fms-like tyrosine kinase 1, or sFlt-1. In a healthy pregnancy, protein levels are balanced, but in preeclampsia, the placenta overproduces sFlt-1.
This excess protein plays a central role in the pathogenesis of the disease, contributing to the systemic inflammation and vascular damage that lead to dangerously high blood pressure and organ dysfunction. Until now, treatment has focused primarily on managing symptoms—like lowering blood pressure or inducing early delivery—rather than targeting the underlying protein driving the condition.
A New Approach: Extracorporeal Apheresis
The recent study tested a strategy to directly deplete circulating sFlt-1 using a process called extracorporeal apheresis. Think of this as a highly specialized filtration system. Blood is taken from the patient, passed through an adsorber containing high-affinity IgG1 antibodies specifically designed to bind to sFlt-1, and then returned to the body.
Before moving to human trials, the team tested this method in pregnant baboons, where the process resulted in an approximate 50% reduction of circulating sFlt-1 levels.
The Human Trial: Safety and Efficacy
The first-in-human trial was a single-arm, open-label study divided into two phases to ensure the treatment was both safe and effective for women with very preterm preeclampsia.
Phase A: Establishing Safety
In the first phase, seven women received single ascending doses of the treatment. The primary goal was safety and tolerability. The results were encouraging: maternal and fetal vital signs, as well as umbilical artery pulsatility indices, remained stable throughout the process. Preapheresis sFlt-1 levels in this group averaged 15,120 ± 4,484 pg/ml.

Phase B: Measuring Impact
The second phase involved nine women with a median gestational age of 30.3 weeks. These patients presented with mean blood pressures of 146 ± 10 mmHg (systolic) and 92 ± 5 mmHg (diastolic), with preapheresis sFlt-1 levels of 11,960 ± 3,056 pg/ml.
The results from Phase B provided critical data on the treatment’s impact:
- Protein Reduction: Each apheresis session reduced sFlt-1 levels by 16.7 ± 7.6%.
- Blood Pressure Drop: Mean arterial pressures decreased by 4.1 ± 7.8 mmHg.
- Direct Correlation: There was a strong correlation (R = 0.63) between the reduction of sFlt-1 and the drop in mean arterial pressure.
Clinical Outcomes and Pregnancy Extension
The ultimate goal of treating preterm preeclampsia is to buy time for the fetus to develop, reducing the risks associated with extreme prematurity. In this trial, pregnancies continued from the time of admission for a median of 10 days, with a range between 3 and 19 days.
Crucially, neonatal birth weights generally remained stable or actually increased among the women who achieved the longest extensions of their pregnancy. This suggests that the therapy doesn’t just manage maternal symptoms but may provide a meaningful window for fetal growth.
- Targeted Action: The therapy uses IgG1 antibodies to selectively remove the sFlt-1 protein from the blood.
- Proven Safety: The procedure was well tolerated, with stable maternal and fetal vital signs.
- Blood Pressure Control: Reductions in sFlt-1 levels strongly correlated with lower mean arterial pressures.
- Pregnancy Extension: The treatment helped extend pregnancies by a median of 10 days, potentially improving neonatal birth weights.
Frequently Asked Questions
Is this treatment available in hospitals now?
No. This was a first-in-human trial designed to provide critical safety data. While the results are promising, larger controlled trials are necessary before this becomes a standard clinical treatment.

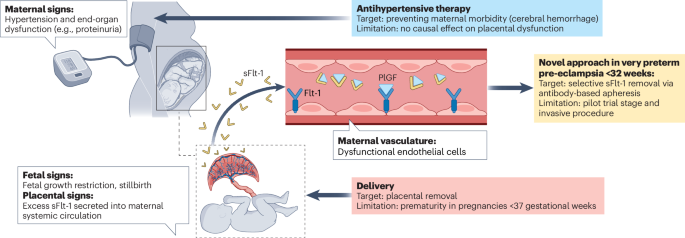
How does this differ from standard preeclampsia treatment?
Standard treatments typically involve antihypertensive medications to manage blood pressure or the delivery of the baby to stop the disease. This approach is “targeted,” meaning it attempts to remove the specific protein causing the disease process.
Are there risks to the baby?
In this trial, fetal vital signs and umbilical artery pulsatility indices remained stable, indicating that the apheresis process was well tolerated by the fetus.
The Path Forward
While this study is small, it marks a pivotal shift in how we approach preeclampsia. By moving from symptom management to targeted molecular removal, we may soon have a tool that can safely extend pregnancies and improve outcomes for both mothers and infants. As research progresses into larger, controlled trials, this “protein-clearing” strategy could become a cornerstone of maternal-fetal medicine.