{kind=link}
Genetic Variants and Dapagliflozin: New Insights into Heart Failure Treatment
Patients with type 2 diabetes who carry rare genetic variants associated with cardiomyopathies (CMP) appear to derive similar cardiovascular benefits from dapagliflozin as those without these variants. According to a secondary analysis of the DECLARE-TIMI 58 trial, the sodium-glucose cotransporter 2 (SGLT2) inhibitor consistently reduced the risk of hospitalization for heart failure (HHF) regardless of a patient’s underlying genetic predisposition to heart muscle disease.
How Genetic Variants Influence Heart Failure Risk
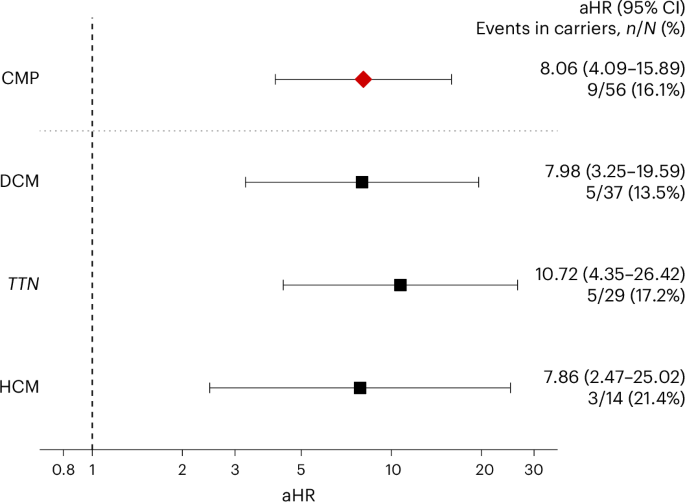
Cardiomyopathies—including dilated (DCM), hypertrophic (HCM), and arrhythmogenic right ventricular (ARVC) cardiomyopathies—are often driven by rare, pathogenic genetic variants. Research published in Nature Medicine indicates that these variants significantly increase the risk of heart failure, independent of traditional diabetes-related factors. In the study, researchers utilized whole-exome sequencing from over 12,000 trial participants to identify individuals carrying pathogenic or likely pathogenic variants in genes linked to these conditions. The data shows that carriers of these variants face a higher baseline risk of hospitalization for heart failure compared to non-carriers, emphasizing the role of genetics in complex metabolic heart disease.

Dapagliflozin Efficacy Across Genetic Profiles
Dapagliflozin remains an effective intervention for patients with type 2 diabetes at risk for atherosclerotic cardiovascular disease, even among those with a high genetic burden for cardiomyopathy. Clinical data from the study demonstrates that the drug’s ability to lower the incidence of HHF is not diminished by the presence of rare CMP-associated variants. While the primary trial confirmed that dapagliflozin reduces cardiovascular death and heart failure hospitalizations overall, this specific analysis suggests that the drug’s mechanism—likely involving improved sodium excretion and reduced cardiac preload—provides robust protection that bypasses the specific genetic triggers of cardiomyopathy.
Why This Matters for Clinical Practice
This finding is significant because it suggests that genetic testing for specific cardiomyopathy variants is not currently required to determine the suitability of SGLT2 inhibitor therapy in diabetic populations. Historically, clinicians have looked toward genetic screening to predict disease progression; however, this study indicates that standard-of-care pharmacotherapy with agents like dapagliflozin offers a “genotype-agnostic” benefit. According to the analysis, the treatment interaction between dapagliflozin and the presence of CMP mutations was not statistically significant, meaning the drug performed reliably across all genetic subgroups studied.
Comparison of Clinical Outcomes
The following table summarizes the observed impact of dapagliflozin on heart failure endpoints as established in the broader DECLARE-TIMI 58 trial, which serves as the foundation for this genetic sub-analysis:
| Outcome | Hazard Ratio (HR) | Confidence Interval (CI) |
|---|---|---|
| CV Death or HHF | 0.83 | 0.73–0.95 |
| Hospitalization for Heart Failure (HHF) | 0.73 | 0.61–0.88 |
Future Directions in Precision Cardiology
While this study confirms that dapagliflozin is a reliable tool for high-risk diabetic patients regardless of their genetic cardiomyopathy status, it also highlights the growing importance of precision medicine in cardiology. Future research will likely focus on whether specific subsets of cardiomyopathy patients—perhaps those with advanced structural disease—might require different, targeted therapeutic approaches. For now, the evidence supports the broad application of SGLT2 inhibitors in patients with type 2 diabetes to mitigate the risk of heart failure, regardless of whether a rare genetic variant is present.
Related reading